- Aminophylline is stable mixture of theophylline (bronchodilator) and ethylene diamine in ratio 2:1. Ethylene diamine makes theophylline more water soluble.
- It is more soluble in water than theophylline but have same pharmacological properties.
- It is methylated xanthine derivative which belongs to a group of bronchodilators. Bronchodilators relax muscle in bronchial tube of lungs, increase flow of air through bronchial tubes and helps to relieve cough, wheezing, troubled breathing and shortness of breath.
Mechanism of action and Pharmacological action of Aminophylline
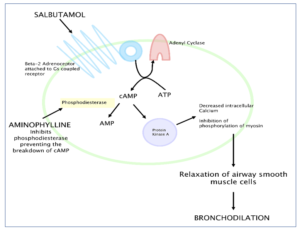
Figure 1- Mechanism of action of aminophylline
- Its exact mechanism of action is not clearly understood. Its mechanism of action is similar to other methylated xanthine derivatives.
- Once it reaches inside the body, theophylline is released. It is competitive nonselective phosphodiesterase inhibitor. It inhibits phosphodiesterase and inhibit conversion of cAMP to inactive 5’ AMP, thus increasing the concentration of cAMP. The increased cAMP promotes catecholamine stimulation and induce release of epinephrine resulting in bronchodilation.
- It also inhibits adenosine receptor in the airways. This results in blocking of adenosine mediated bronchoconstriction in inflammatory states.
- It inhibits late response to allergens. Theophylline also activate histone deacetylase to prevent transcription of inflammatory genes.
- It acts synergistically with beta adrenergic agonists like salbutamol, salmeterol etc.
Pharmacokinetics of Aminophylline
- When administered through oral route, it undergoes first pass metabolism, so it is less effective. Its absorption is slowed when administered with food.
- It can be administered through IV route. For IV aminophylline, a loading dose given slowly (20-20 minutes) is followed by a maintenance infusion.
- Also available as rectal suppository and extended release tablet form.
- Around 60 % of drugs bind to protein.
- Half-life is about 7-9 hours.
Therapeutic Uses of Aminophylline
In acute attack of asthma
- Short acting beta-2 adrenergic receptor agonist (SABA) like salbutamol and fenoterol are first line agent in treating acute attack of asthma. If inhaled SABA treatment cannot produce relief from acute asthma attack within 0.5-1-hour, aminophylline is administered by IV infusion in 5% glucose in a dose of 5 mg/kg over 15-30 minutes, followed by 0.5-1 mg/kg per hour for several hours.
- Large dose may be required in case of smokers.
In chronic persistent asthma
- Slow release oral preparation is useful in chronic persistent asthma.
Some other uses are:
- In COPD (Chronic Obstructive Pulmonary Disease) in combination with beta-adrenergic agonists.
- To reverse dipyridamole induced adverse effects during stress myocardial perfusion imaging (MPI).
- Treatment option for anaphylactic shock.
- Prophylactic use to prevent apnea in higher risk pre-term infants.
Adverse Effects
- Aminophylline has narrow therapeutic index.
- Cardiac toxicity includes sinus tachycardia, ventricular tachycardia, supraventricular tachycardia, ventricular fibrillation, ventricular premature beats and multifocal atrial tachycardia. Dilation of vascular smooth muscle can cause headache, flushing and hypotension.
- GI irritation includes nausea, vomiting and anorexia.
- It may affect CNS and cause insomnia, agitation, anxiety and fits.
- Rarely (less than 0.1%) it can cause allergic reaction; hives, skin rashes, difficulty in breathing or swelling of lips, throat and mouth.
- Hyperkalemia, hyperglycemia and acid/base disturbance may occur.
Note- The majority of aminophylline medications are discontinued and the remaining medications on the market are in short supply due to their narrow therapeutic index.
Drug Interaction
- Drugs which increase serum theophylline concentration by decreasing its metabolism include:
- Cimetidine
- Thiabendazole
- Tacrine
- Enoxacin
- Drugs which decrease serum aminophylline concentration by accelerating its metabolism include;
- Phenobarbital
- Carbamazepine
- Rifampin
- Smoking increases breakdown of theophylline.
- It is excreted in breast milk and may cause irritation and mild toxicity in nursing infants.
Dietary instruction
- Having food containing high amount of caffeine, tea and cocoa may increase side effects of aminophylline so such foods (in large amount) should be avoided while in aminophylline medication.
- Avoid excessive or chronic alcohol consumption as it may reduce aminophylline clearance and increase its serum concentration.
Contraindication
- It should be contraindicated in patients allergic to aminophylline or theophylline.
- Used with caution in kids below 3 months age.
- Used with caution in patient with liver disease, stomach ulcer and seizure or history of seizure.
References
- https://medlineplus.gov/druginfo/meds/a601015.html
- https://www.drugbank.ca/drugs/DB01223
- https://www.medicinenet.com/aminophyllineinjection/article.htm#what_is_aminophylline_and_how_does_it_work_mechanism_of_action
- Cooney L, Sinha I, Hawcutt D. Aminophylline Dosage In Asthma Exacerbations in Children: A Systematic Review. Plos One.
- Lin LF, Cheng CY, Hou CH, Ku CH, Tseng NC, Shen DHY. Experience of Low-Dose Aminophylline Use to Relieve Minor Adverse Effects of Dipyridamole in Patients Undergoing Stress Myocardial Perfusion Imaging. J Nucl Cardiol. 2014; 21(3): 563-9.
- Komadina KH, Carlson TA, Strollo PJ, Navratil DL. Electrophysiologic Study of the Effects of Aminophylline and Metaproterenol on Canine Myocardium Chest Journal. 1992; 101 (1): 232–238.
- Armanian AM, Badiee Z, Afghari R, Salehimehr N, Hassanzade A, Sheikhzadeh S, Tehrani MS, Rezvan G. Prophylactic Aminophylline for Prevention of Apnea at Higher-Risk Preterm Neonates. Iran Red Crescent Med J. 2014; 16(8): e12559.
- A Textbook of Clinical Pharmacology and Therapeutics.
- Pharmacology and pharmacotherapeutics. 24th edition.