- Aspirin or acetyl salicylic acid is the most commonly used salicylate and belongs to class of NSAIDs.
- It is one of the most widely used medication all over the world. It is included in WHO list of essential medicines. and is also available as generic medicine. In 2017, it was 42nd most commonly prescribed medication in United States.
- Red Edmund Stone discovered a precursor to aspirin in bark of willow tree . It was first synthesized by Hoffman in 1898. Heinrich Dreser – Bayer’s chief pharmacologist give the name ‘aspirin’.
Mechanism of action
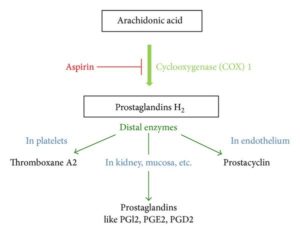
Figure 1- Mechanism of action of Aspirin
- During pain, inflammation and fever, arachidonic acid is liberated from phospholipid fraction of cell membrane by phospholipase A2. Arachidonic acid is converted to prostaglandins (PGs) by cyclooxygenase (COX-1 and COX-2).
- The prostaglandins produced sensitize blood vessels to other inflammatory mediators which increase permeability and sensitize chemical receptor of afferent pain ending to mediators such as histamine and bradykinin. PGE2 and PGI2 produce hyperalgesia associated with inflammation. They are also involved in pyretic response.
- Aspirin is a weak organic acid which irreversibly inactivates cyclooxygenase by acetylating it (by transferring its acetyl group).
- The inactivation of cyclooxygenase inhibits production of prostaglandins from arachidonic acid. This results in analgesic, anti-pyretic and anti-inflammatory action of aspirin.
Pharmacological Actions
Analgesic action
- Aspirin produces relief of pain without hypnosis or impairment of mental activity. It is useful in dull pain, throbbing pain, toothache and dysmenorrhea.
- However, it is not useful in visceral pain or deafferentation pain.
Anti-pyretic action
- In case of fever, it resets thermostatic mechanism to normal level by increasing dissipation of heat by producing cutaneous vasodilation and sweating. This results in rapid reduction of the body temperature.
- It doesn’t reduce heat production and also doesn’t lower body temperature in normal individual.
Anti-inflammatory action
- It possesses anti-inflammatory properties when used in high doses. Hence, it helps to reduce inflammation in arthritis.
-
Respiratory stimulation
- Aspirin increases oxygen consumption and CO2 production (especially in skeletal muscle) and hence, stimulate respiration. It also stimulates chemoreceptors and stimulate medullary respiratory center directly.
- This may result in respiratory alkalosis.
Anti-platelet activity
- Inhibition of COX by aspirin inhibit synthesis of thromboxane A2 (TXA2) in platelets and inhibits platelet aggregation. Thus, a standard tablet dose of aspirin can approximately double the mean bleeding time in normal person for about 4-7 days.
Acid-base and electrolyte balance and renal effect
- Therapeutic dose of aspirin produce change in acid-base balance and electrolyte pattern. To compensate respiratory alkalosis, bicarbonates are excreted in urine along with increased sodium and potassium excretion. This is the reason behind renal acidosis after intensive aspirin therapy.
- It causes retention of salt and water. In therapeutic dose, it doesn’t affect renal function. However, it can affect renal function by inhibiting COX-1 enzymes in patients with renal disease or hypovolemia.
Cardiovascular effects
- In therapeutic doses, it doesn’t cause any harmful effect on CVS. Low dose of aspirin is recommended for its cardioprotective effects.
- Administration of high dose for prolonged period can produce non-cardiogenic pulmonary edema in older patients. it may cause rise in BP due to sodium and water retention.
GI effects
- Aspirin causes loss of protective action of PGE on stomach and cause epigastric distress, gastric ulceration, exacerbation of peptic ulcer symptoms, erosive gastritis and gastric hemorrhage. It also causes nausea, vomiting, gastric bleeding leading to melena.
Hepatic effects
- Aspirin doesn’t modify hepatic function in therapeutic dose. High dose can cause hepatic injury, particularly in children. The injury is reversible on discontinuation of aspirin.
Metabolic effects
- In toxic doses, it may cause increased protein catabolism, hyperpyrexia and negative nitrogen balance.
- When used in some diabetic patients, it may inhibit neoglucogenesis and enhance peripheral utilization of glucose leading to reduced blood sugar level and glycosuria. In normal individuals, large doses can produce hyperglycemia.
- It reduces lipogenesis. Toxic dose lead to formation of ketone bodies.
Uricosuric effects
- In small doses (1-2 gm/day), it decreases urate secretion and increases plasma urate level. It blocks effect of uricosuric agents like probenecid.
- When used in large doses (more than 5 gm/day), it induces uricosuria and reduce plasma urate level.
Local effect
- It possesses antiseptic, fungistatic and keratolytic actions. Salicylic acid has irritant action on skin and mucosa and destroy epithelial cells.
- Due to its keratolytic action, it is effective in warts, corns and fungal infection.
Pharmacokinetics
- After oral administration, it is absorbed rapidly from small intestine. Its absorption is delayed by presence of food. It is distributed throughout body tissues and fluids after its absorption.
- It undergoes rapid metabolism (50-60%) to salicylate by deacetylation during first pass and is further hydrolyzed into salicylic acid in tissues and blood.
- Around 80-90% of aspirin bind to proteins, especially albumin.
- At lower dose (300-600 mg), it follows first order kinetics and plasma level increase with increase in dose. At higher dose (1-2 gm), it follows zero order kinetics and increase in plasma level is irregular which can cause severe toxicity.
- The plasma half-life is around 20 minutes. At higher dose, half life may increase to around 15-30 hours.
- It is mainly excreted in urine. It crosses placental barrier.
Therapeutic Uses
- It is widely used as analgesic (in headache, dysmenorrhea, neuralgia and myalgia) and anti-pyretic.
- Used as anti-inflammatory drug in high doses. Hence, used to treat osteoarthritis, gout and rheumatoid arthritis.
- Used in large dose in acute rheumatic fever to produce relief from pain and inflammation.
- it is used as anti-platelet agent.
- Combination of aspirin with opioids can be used to reduce pain in malignancy.
- Low dose may be used prophylactically to prevent stroke and myocardial infarction in patients at high-risk (who had already suffered from stroke or heart attack). However, its prophylactic use in low-risk or normal people is not recommended as hazards of aspirin approximately balance the benefits.
Adverse Effects
- Allergic or pseudo allergic reactions include skin rashes, urticaria, pruritus, angioedema, thrombocytopenic purpura and anaphylactoid reaction.
- It can induce idiosyncratic, mild hemolysis in individuals with G6PD deficiency.
- Common side effects include nausea, vomiting, dyspepsia, heartburn and ulceration. Gastric bleeding is very common which may be due to platelet inhibition, local mucosal action and hypoprothrombinemia.
- Prolonged therapy even with low dose can cause anemia.
- Reye’s syndrome– it occurs when aspirin is administered to children below 12 years suffering from viral infection, especially influenza. It is characterized by acute encephalopathy and fatty liver.
Overdose
- Overdose may be acute or chronic. Acute poisoning occurs due to a single large dose and has a mortality rate of 2%. Chronic poisoning occurs due to higher than normal doses taken over prolonged period and is more lethal, with a mortality rate of 25%.
- Patients with mild toxicity may have nausea and vomiting, abdominal pain, lethargy, tinnitus, and dizziness. Severe poisonings may cause more fatal signs and symptoms include high body temperature, fast breathing rate, respiratory alkalosis, metabolic acidosis, low blood potassium, low blood glucose, hallucinations, confusion, seizure, cerebral edema, and coma. The most common cause of death following an aspirin overdose is cardiopulmonary arrest usually due to pulmonary edema.
Drug interaction
- Aspirin act synergistically with coumarin anti-coagulants and increases risk of bleeding.
- As it is highly protein bound drug, it can be displaced from protein binding sites by some drugs. It also displaces some highly protein bound drugs like phenytoin, warfarin, antidiabetic drugs like tolbutamide and chlorpropamide and valproic acid.
- It inhibits absorption of vitamin C.
- Co-administration with anti-inflammatory painkiller like ibuprofen and naproxen, SSRIs (selective serotonin reuptake inhibitor) antidepressant like citalopram and alcohol intake increase risk of GI bleeding.
Contraindication
- It should not be used in children below 12 years age.
- When used in pregnancy, it delays onset of labor and cause greater blood loss at delivery. It cross placental barrier and may cause hyperpnoea and hemorrhage in newborn. So, it is avoided in pregnancy. Low dose may be safe.
- It should not be used in following conditions:
- Contraindicated in person allergic to aspirin or salicylic acid.
- In patients with peptic ulcer.
- Contraindicated in hemophilia or other bleeding disorder.
- In person who drink alcohol regularly.
- In person undergoing any surgery, use of aspirin should be stopped 7 days prior to surgery as it increases risk of serious bleeding.
References
- Undas A, Brummel-Ziedins KE, Mann Antithrombotic properties of aspirin and resistance to aspirin: beyond strictly antiplatelet actions. Blood. 2007; 109(6): 2285–2292.
- Ruiz IF. Aspirin for primary prevention of CVD: a matter of balance. Nature Reviews Cardiology. 2018; 15: 651.
- Chubak J, , Whitlock EP, Williams SB, , Aruna Kamineni A, Burda BU, Buist DSM, Anderson ML. Aspirin for the Prevention of Cancer Incidence and Mortality: Systematic Evidence Reviews for the U.S. Preventive Services Task Force. Ann intern Med. 2016; 164(12): 814-825.
- Fuster V, Sweeny JM. Aspirin A Historical and Contemporary Therapeutic Overview. Circulation. 2011; 123: 768–778.
- Vane JR, Botting RM. The Mechanism of action of Aspirin. Thrombosis Research. 2003; 110: 255–258.
- Goodman and Gillman’s Manual of Pharmacology.
- Pharmacology and pharmacotherapeutics. 24th edition.
- A Textbook of Clinical Pharmacology and Therapeutics.
- Lippincott Illustrated Reviews Pharmacology, 6th edition