
- Tetracyclines are broad spectrum antibiotics, discovered in the 1940s. Chlortetracycline is the first tetracycline to be identified. It was isolated from Streptomyces aureofaciens.
- Tetracyclines are napthacene derivatives consisting of four fused rings with a variety of functional groups attached. It has been used extensively over the last 50 years to treat bacterial infection in both human beings and animals.
- Tetracyclines can be natural or semi-synthetic. Some examples of natural tetracyclines are chlortetracycline, oxytetracycline and tetracycline itself. Examples of semi-synthetic tetracyclines are methacycline, doxycycline, minocycline, demeclocycline and tigecycline
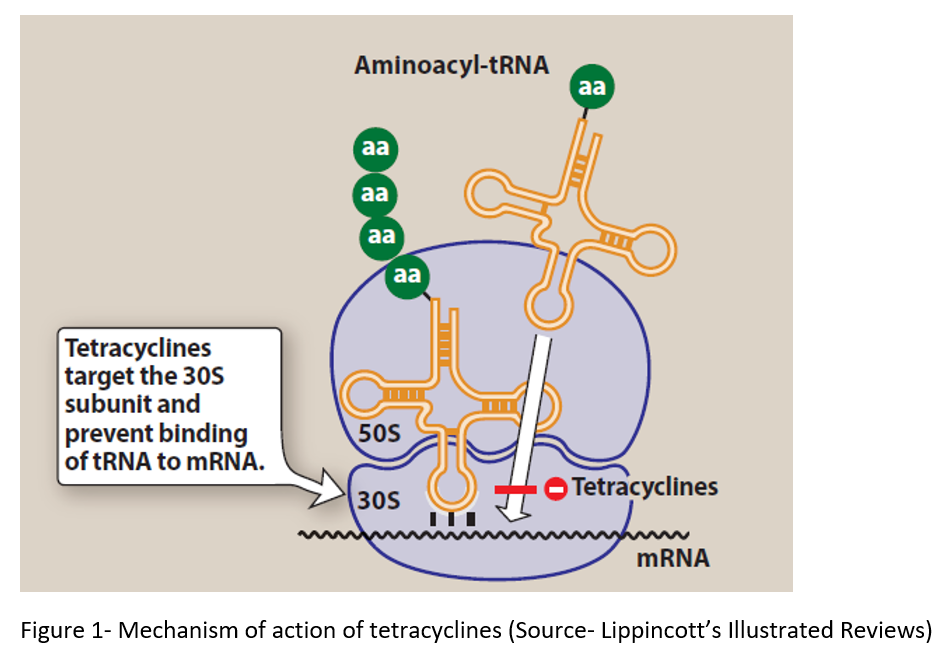
Mechanism of action of Tetracyclines
- Tetracyclines enter susceptible organisms via passive diffusion and energy dependent transport mechanism.
- They bind to 30S ribosomal subunit and block aminoacyl transfer RNA from attaching to acceptor site on the mRNA-ribosomal complex. Thus, they inhibit protein synthesis.
- They also chelate calcium and magnesium ions which may help in its action.
Spectrum of antibacterial activity
- Tetracyclines are bacteriostatic effective against wide range of aerobic and anaerobic gram-positive and gram-negative bacteria. They are more active against gram-positive bacteria than gram-negative bacteria.
- They are also effective against rickettsial organisms, chlamydia, protozoa like E. histolytica and plasmodia and actinomycetes.
Pharmacokinetics of Tetracyclines
- They are administered through oral, parenteral and local route. Local route is preferred in eye only. Tetracyclines are adequately absorbed after oral administration. Administration along with calcium and magnesium containing compounds like milk and antacids may interfere with their absorption. It is due to formation of non-absorbable chelates.
- They are mainly absorbed from duodenum and upper small intestine, are widely distributed in the various body parts and body fluids. They can cross placental barrier and are secreted in milk. And they remain concentrated in bone marrow, liver, spleen, lungs and enamel of unerupted teeth.
- Their half-life is in the range of 6-12 hours and are administered 2-4 times daily.
- They are metabolized in liver. Most of them are excreted through kidney in the form of urine except doxycycline and minocycline. Some amount is also excreted in bile.
Clinical Uses of Tetracyclines
- Used to treat rickettsial infections like typhus, rocky mountain spotted fever and Q fever. Relapses are rare.
- In bacillary infection like brucellosis and tularemia.
- In primary atypical pneumonia caused by Mycoplasma pneumonia.
- To treat chlamydia infections like trachoma, non-gonococcal urethritis (NGU), inclusion conjunctivitis and cervicitis.
- Doxycycline is effective in treating cholera.
- To treat acne.
- They are also used to treat infections in poultry, cattle, sheep and domestic pets. Also used in animal food as growth promoters.
Adverse Effects
- Nausea, vomiting, GI irritation and loose stools are common. Nausea and vomiting may be prevented by taking drugs after food.
- Severe sunburn or phototoxicity may occur in patients taking tetracyclines when exposed to sun or ultraviolet rays. This is more common with doxycycline and demeclocycline.
- In patients receiving large dose of tetracycline over short period, hepatic dysfunction may occur. Pregnant women are more susceptible to this.
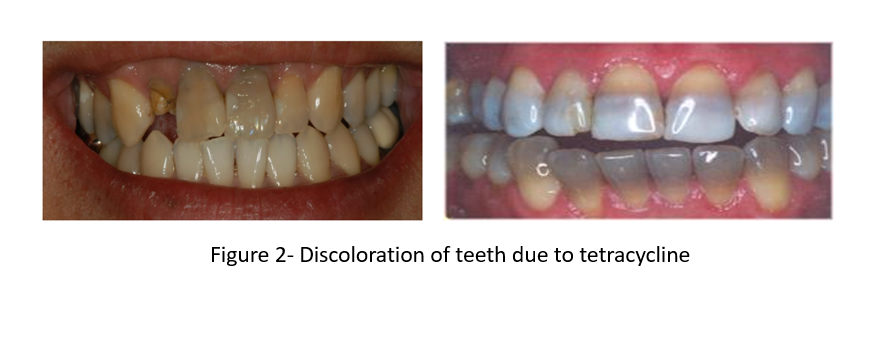
- Tetracycline gets deposited in bones and teeth. In children, they may cause discoloration and hypoplasia of teeth and temporary cessation of growth. When used in pregnant women, may lead to yellow staining of teeth of infant. This discoloration of teeth is permanent.
- Allergic reactions like skin rashes, angioedema, anaphylaxis is rare.
- Prolonged tetracycline therapy can suppress normal intestinal flora and cause superinfection. Infection with Candida albicans, S. aureus and Clostridium difficile are common.
- They may aggravate azotemia in patients with renal impairment.
Contraindication
- They shouldn’t be used in pregnancy or breastfeeding woman. If it is administered during pregnancy, it gets deposited in fetal bones and may reduce their linear growth.
- They are avoided in infants and in children up to 12 years age.
Tetracycline Resistance
- Main mechanisms for resistance are decreased accumulation of tetracycline, enzymatic inactivation of tetracyclines and production of ribosomal protein that displaces tetracycline from its target. Cross resistance among tetracyclines depend on which mechanism is involved in resistance.
- Organisms including H. Influenzae, E. Coli, Pneumococci, Staphylococci and group A Streptococci show resistance.
- Gram-positive bacteria resistant to tetracycline are susceptible to chloramphenicol whereas gram negative bacteria resistant to tetracycline are resistant to chloramphenicol as well.
Potential of Tetracyclines in Treatment of COVID-19
- Tetracycline are highly lipophilic which can chelate zinc compounds on matrix metalloproteinases (MMPs). Coronaviruses highly rely on host MMPs for survival, replication, cell-to-cell adhesion. Thus, tetracycline may limit replication of COVID-19 and help in inhibiting COVID-19 infection in human.
- The cytokine levels are found to be elevated during infection with corona virus. Tetracycline possess anti-inflammatory properties and helps in decreasing level of inflammatory cytokines.
- Significant number of patients suffering from COVID-19 develop complicated pneumonia or acute respiratory distress syndrome (ARDS). Tetracycline may be helpful to decrease death and alleviate hospital load in such complications.
- Further research is required to investigate potential of tetracycline in treating COVID-19.
References
- https://accpjournals.onlinelibrary.wiley.com/doi/10.1002/phar.2395
- Griffin MO, Fricovsky E, Ceballos G, Villarreal F. Tetracyclines: a pleitropic family of compounds with promising therapeutic properties. Review of the literature. Am J Physiol Cell Physiol. 2010 Sep; 299(3): C539–C548.
- Chopra I, Roberts M. Tetracycline Antibiotics: Mode of Action, Applications, Molecular Biology, and Epidemiology of Bacterial Resistance. Microbiol Mol Biol Rev. 2001 Jun; 65(2): 232–260.
- Nelson ML, Levy SB. The history of the tetracyclines. Ann. N.Y. Acad. Sci. 1241 (2011) 17–32.
- Goodman and Gillman Manual of Pharmacology and Therapeutics.
- Lippincott Illustrated Reviews Pharmacology, 6th edition.
- Pharmacology and pharmacotherapeutics. 24th edition.