
Chloramphenicol
- Chloramphenicol is broad spectrum antibiotic derived from Streptomyces venezuelae. It was introduced into clinical practice in 1949. Chloramphenicol was the first antibiotic to be manufactured synthetically on large scale.
Mechanism of action of Chloramphenicol
- It penetrates readily into bacterial cell, bind reversibly to 50S ribosomal subunit and block fundamental ribosomal activities, such as peptidyl transferase activity and translation termination. Thus, it inhibits synthesis of bacterial proteins.
Spectrum of antibacterial activity
- Chloramphenicol is effective against variety of gram-positive bacteria, gram-negative bacteria and anaerobes. It acts as bacteriostatic against broad spectrum of bacteria and bactericidal against H. influenzae, S. pneumoniae and Neisseria Meningitidis.
- It is active against Chlamydia, Rickettsia and Mycoplasma.
Pharmacokinetics
- The most commonly used preparations of are crystalline powder for oral administration, palmitate ester for oral administration as a suspension and a succinate ester for parenteral administration. Both esters are inactive and require hydrolysis for anti-bacterial activity.
- Blood level of chloramphenicol after oral administration is superior than after IM administration.
- The time for peak plasma concentration depends on particle size and invitro dissolution and deaggregation rates. About 60 % of plasma chloramphenicol is bound to protein. The drug is distributed to many tissues and fluid including CSF (Cerebrospinal Fluid) and breast milk. It can cross placenta.
- It is metabolized mainly in liver. Glucuronide is the major metabolite formed. About 5-15 % of chloramphenicol is excreted unchanged in urine.
Clinical Uses
It should be used to treat infections in which its benefits outweigh the risks of potential toxicities.
- In typhoid fever and bacterial meningitis.
- In rickettsial diseases and brucellosis patients who are allergic to tetracycline or in whom tetracycline is contraindicated.
- Also in ocular infections.
- In plague.
Adverse Effects
- It inhibits the protein synthesis of the inner mitochondrial membrane which can cause adverse effects. Because of its potential adverse effects, its use is limited in USA.
- Skin rashes, drug fever, exfoliative dermatitis have been reported.
- The major side effects are irreversible bone marrow suppression, aplastic anemia and leukemia. Aplastic anemia may occur due to prolonged treatment or repeated courses. Its incidence is between 1:10,000 and 1:100,000.
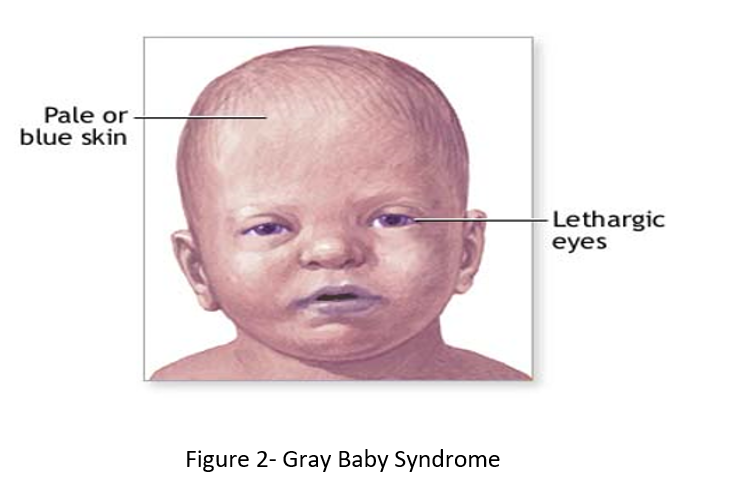
- Gray baby syndrome is observed in neonates and infants. The initial symptoms are vomiting, lethargy and anorexia. Later, the condition worsens leading to hypothermia, gray cyanosis, shock and finally death. It occurs because neonates and infants lack fully functional liver enzymes and thus chloramphenicol remains unmetabolized.
- Effects in CNS like headache, mental confusion, depression, delirium is reported. Optic neuritis may occur rarely. It may affect cochlear function, if used locally for ear infection
- In patients with typhoid fever, if used in large loading dose a ‘typhoid shock’ syndrome may develop. Liver damage is rare.
Chloramphenicol Resistance
- Resistance to chloramphenicol is mainly due to production of chloramphenicol acetyl transferases (CAT), an inactivating enzyme. Other mechanisms of resistance are permeability barriers and efflux system inactivation by phosphotransferases mutations.
- Some Enterococcus faecium and Pseudomonas aeruginosa strains are resistant to chloramphenicol. Some Veillonella spp. and Staphylococcus capitis strains have also developed resistance to chloramphenicol to varying degrees.
References
- Balbi HJ. Chloramphenicol A review. Pediatrics in Review. 2004; 25(8): 284-8.
- Madhavan HN, Bagyalakshmi R. Farewell, Chloramphenicol? Is this True?: A Review. RRJMB. 2014; 3(1): 13-26.
- Drugs during pregnancy and lactation. 2nd edition.
- Pharmacology and pharmacotherapeutics. 24th edition.
- Goodman and Gillman Manual of Pharmacology and Therapeutics.
- Lippincott Illustrated Reviews Pharmacology, 6th edition.
- https://www.ncbi.nlm.nih.gov/books/NBK555966/