- Succinylcholine also known as suxamethonium or suxamethonium chloride is a quaternary ammonium compound. It is a depolarizing agent with short term muscle relaxing properties.
- It is the only depolarizing muscle relaxant in use nowadays. Its structure resembles two molecules of acetylcholine (ACh) joined together.
- Succinylcholine was first discovered in 1906 and was introduced in medical field in 1951. It is also available as generic medicine. It is included in World Health Organization’s List of Essential Medicines.
Mechanism of action of succinylcholine
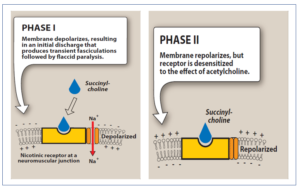
Figure 1- Mechanism of action of succinylcholine (Source- Lippincott’s Illustrated Reviews)
- It binds to nicotinic receptor, acts as partial agonist of acetylcholine and depolarize the junction. In contrast to ACh, which is instantly metabolized by acetylcholinesterase enzyme (AChE), succinylcholine is destroyed more slowly as it is susceptible only to liver and plasma pseudocholinesterase. This causes persistent depolarization during which muscles are insensitive to ACh and remain paralyzed.
- It first causes opening of sodium channel associated with nicotinic receptors leading to depolarization of receptor (Phase I). This leads to transient twitching of muscle (fasciculation). Continued binding makes the receptor incapable of transmitting further impulse. Continuous depolarization leas to gradual repolarization as sodium channel closes or is blocked. This Causes resistance to depolarization (Phase II) and lead to flaccid paralysis.
Pharmacological actions of succinylcholine
Skeletal Muscle
- It produces paralysis of skeletal muscle. It can affect respiratory muscle and produce transient apnea in its peak level.
- The skeletal muscle paralysis is enhanced by antiChE neostigmine which increases local concentration of ACh.
Cardiovascular system
- On repeated administration, it stimulates vagal nuclei and sympathetic ganglia. Stimulation of vagal nuclei can cause to bradycardia, hypotension and cardiac arrhythmia whereas sympathetic ganglia stimulation can cause persistent hypertension and tachycardia.
Miscellaneous
- In large doses, it exerts muscarinic effect and can cause hypotension. Atropine is generally given before it due to its muscarinic effect.
- Due to prolonged depolarization, potassium may shift from intracellular space to extracellular leading to hyperkalemia.
Pharmacokinetics of succinylcholine
- It is given through IV route. Muscle fasciculations last for 10-15 seconds, peak effect may occur within 1-2 minutes and muscle power recovers within 5 minutes.
- Its short duration of action is due to redistribution and rapid hydrolysis by pseudocholinesterase. So, it is given by continuous infusion if longer duration of action is required.
- It is hydrolyzed by liver and plasma pseudocholinesterase to succinic acid and choline. About 10% is excreted unchanged in urine.
- It crosses placental barrier.
Therapeutic Uses
- It is useful when rapid endotracheal intubation is required during induction of anesthesia. (Because of its rapid action, aspiration of gastric contents can be avoided during intubation). Thus, it is useful adjuvant to anesthesia during abdominal surgery and brief procedures like bronchoscopy, laryngoscopy and esophagoscopy.
- Used during electroconvulsive therapy. It is used with diazepam to protect the patient from injury.
Adverse Effects
- Most common reported adverse effects are masseter muscle rigidity (MMR), malignant hyperthermia, myalgia and hypotension. MMR can lead to failed laryngoscopy and endotracheal intubation. Myalgia is sometimes accompanied by muscle stiffness and may last for several days producing significant discomfort.
- Hyperkalemia may occur rarely. It causes release of potassium from intracellular stores. In patients with burn, massive tissue damage or with other conditions which cause hyperkalemia, this can be life-threatening.
- Large dose may produce apnea. Apnea which require respiratory support for more than 15 minutes is considered abnormal. Certain factors like presence of a hereditary, abnormal plasma pseudocholinesterase, having a poor ability to hydrolyze succinylcholine, or acquired deficiency of normal pseudocholinesterase (in liver disease) and metabolic acidosis also precipitate succinylcholine apnea. Therefore, minimum effective dose of succinylcholine is used that provokes only a short apnea time.
- Succinylcholine- halothane combination can cause cardiac arrhythmia and cardiovascular collapse (rarely).
Drug Interactions
- Concurrent administration in patients taking digitalis or diuretics can cause serious arrhythmia.
- Cyclophosphamide prolong action of succinylcholine and increase duration of its paralyzing effect.
- It act synergistically with various drugs including general anesthetics, anti-cholinesterase drugs, chloroquine, aminoglycosides, calcium channel blockers and catecholamines.
Contraindications
- It should be contraindicated in patients allergic to succinylcholine.
- It should be contraindicated in patients with high level of potassium in blood, burn or other conditions which can lead to hyperkalemia.
- Contraindicated in patients with anemia, myasthenia gravis or cancer.
- Should be contraindicated in Duchenne muscular dystrophy.
- Contraindicated in glaucoma.
- Should be used with caution in severe liver disease and renal disease.
References
- https://www.webmd.com/drugs/2/drug-154320/succinylcholine chlorideintravenous/details/list-contraindications
- Larijani GE, Gratz I, Silverberg M, Jacobi AG. Clinical pharmacology of the neuromuscular blocking agents. 1991; 25(1): 54-64.
- Putzu A, Tramer MR, Giffa M, Czarnetzki C. The optimal dose of succinylcholine for rapid sequence induction: a systematic review and meta-analysis of randomized trials. BMC Anesthesiology. 2020; 20(54): 1-9.
- Sheikh M, Riaz A, Umair H M, et al. (July 24, 2020) Succinylcholine-Induced Masseter Muscle Rigidity Successfully Managed with Propofol and Laryngeal Mask Airway: A Case Report and Brief Review. Cureus. 2020; 12(7): e9376.
- Schreiber J, Lysakowski C, Buder TF, Tramer MR, Prevention of Succinylcholine-induced Fasciculation and Myalgia: A Meta-analysis of Randomized Trials. Anesthesiology. 2005; 103: 877-884.
- Bohringer C, Moua H, Liu H. Is There Still a Rolefor Succinylcholine in Contemporary Clinical Practice?. Transl Perioper & Pain Med. 2019; 6(4):129-135
- Pharmacology and Pharmacotherapeutics. 24th edition.
- Lippincott Illustrated Reviews Pharmacology. 6th edition.