
- Diuretics are drugs that promote diuresis (increased production of urine). Diuretics are mainly used to promote water loss.
- Loop diuretics are among the different types of diuretics. They get this name because of their action on loop of Henle. They are also known as high ceiling diuretics as they are highly effective among all diuretics in mobilizing Na+ and Cl– from the body.
- Furosemide is the most commonly used loop diuretics. Some other examples are bumetanide, torsemide and ethacrynic acid.
Mechanism of Action of Loop diuretics
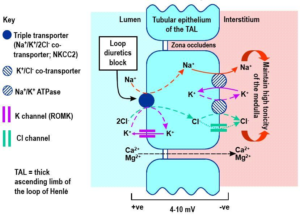
Figure 1- Mechanism of action of loop diuretics
- They primarily act on thick ascending limb of loop of Henle. They inhibit a protein called Na+/K+/2Cl– transporter which is responsible for sodium, potassium and chloride transport. This results in decreased reabsorption of these ions and thus increase urine production.
- As reabsorption of 25-30% of filtered NaCl takes place in ascending limb, loop diuretics have greatest effect among all diuretics.
- Loop diuretics also cause dilatation of capacitance veins which reduce preload and enhance contractile ability of cardiac muscles.
- It also increases PGE2 synthesis in kidney which possess locally protective, vasodilator effect.
Pharmacological Actions of loop diuretics
Kidney
- Its intense diuretic action starts within an hour of oral administration and lasts for around 4-6 hours. Also causes marked sodium, potassium, chloride and phosphate loss.
- Loop diuretics are potent renin releasers. Furosemide cause little change in urinary pH.
- Glomerular Filtration Rate is not affected.
Blood vessels and blood pressure
- Furosemide when administered through IV route dilates peripheral blood vessels, lower arterial BP and reduces cardiac preload and afterload.
Metabolic actions
- Furosemide increases calcium and magnesium excretion. It can cause hyperglycemia and hyperuricemia.
Pharmacokinetics of loop diuretics
- They are administered through oral or parenteral route. Rapidly absorbed from the GI tract (60-100%).
- They have quick onset of action and acts for short duration. Furosemide is excreted within 4 hours by glomerular filtration and tubular secretion. When given through IV route, action begins within 2 minutes and lasts for around 2-3 hours.
- They bound extensively to plasma proteins.
- Around 50 % of furosemide is excreted unchanged in urine. Remaining drug undergoes glucuronide conjugation in kidney. So, elimination half-life is prolonged in patients with renal disease. Bumetanide and torsemide undergoes hepatic metabolism so their elimination half-life is prolonged in hepatic patients.
Therapeutic Uses
- As a very effective, potent and safe diuretic.
- In patients with pulmonary edema.
- In acute and chronic renal failure.
- To induce forced diuresis in barbiturate poisoning.
- As an anti-hypertensive.
- IV furosemide with normal saline infusion is useful in emergency management of hypercalcemia.
- Used in treatment of hyperkalemia.
Adverse Effects
- Loop diuretics severely reduce blood volume which can cause hypotension, shock and cardiac arrythmia.
- Chances of hypokalemia, hypomagnesemia remain. Hyperglycemia and hyperuricemia may occur.
- They can cause ototoxicity characterized by sense of fullness in ear, hearing impairment, deafness and vertigo. Hearing impairment and deafness are reversible. Ethacrynic acid induces ototoxicity more often compared to other loop diuretics.
- Weakness, fatigue, dizziness, cramps and orthostatic hypotension may occur.
- Less common side effects include skin rashes, nausea, diarrhea, thrombocytopenia and neutropenia.
Drug Interaction
- They increase risk of ototoxicity and nephrotoxicity in patients taking aminoglycosides and increase potential for nephrotoxicity and electrolyte imbalance when administered with amphotericin B.
- They increase plasma level of drugs like lithium, propranolol. Also increase activity of anticoagulant drugs.
- Chances of hyperglycemia increase when combined with sulfonyl urea.
- When given with high doses of salicylate (aspirin), may induce salicylate toxicity.
Contraindications
- Contraindicated in patients with dehydration or severe hypovolemia.
- Should be used with caution in patients with hepatic encephalopathy.
References
- Oh SW, Han SY. Loop Diuretics in Clinical Practice. Electrolyte Blood Press. 2015; 13(1): 17–21.
- Marciniak TA. What are the pharmacodynamics of loop diuretics? European Heart Journal – Cardiovascular Pharmacotherapy. 2019; 5(4): 246–248.
- https://pharmafactz.com/loop-diuretics-pharmacology/
- Lippincott Illustrated Reviews Pharmacology, Edition 6th.
- Pharmacology and pharmacotherapeutics, Edition 24th.
- Goodman and Gillman Manual of Pharmacology and Therapeutics.