
- Venlafaxine is SNRI (Selective Serotonin and Nor-adrenaline Reuptake Inhibitor) popularly used as antidepressant. It received approval for medical use in 1993. Chemically, it is bicyclic phenylethylamine compound.
- Some other commonly used SNRIs include:
- Duloxetine
- Desvenlafaxine
- Levomilnacipran
Indications of Venlafaxine
- It’s major uses include management of major depressive disorder. It may be effective in depressed patients resistant to SSRIs (Selective Serotonin Reuptake Inhibitor). Depression is also accompanied by painful symptoms due to modulation of serotonin (5-HT) and nor-epinephrine (NE) in CNS and venlafaxine may also be helpful in reducing this pain.
- Other official uses include generalized anxiety disorder, social anxiety disorder and panic disorder. It is used as monotherapy or in combination with other drugs.
- Some of its off-label uses are migraine prevention, post- traumatic stress disorder, fibromyalgia, obsessive compulsive disorder (OCD), diabetic nephropathy, attention deficit disorder and premenstrual dysphoric disorder.
Mechanism of action of Venlafaxine
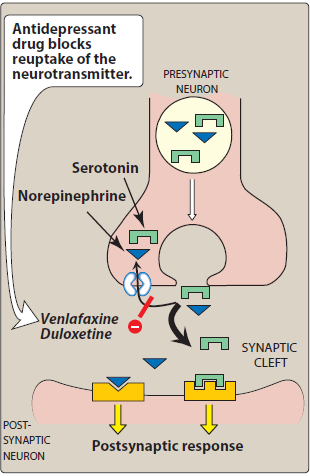
Figure – Mechanism of action of Venlafaxine (Source- Lippincott’s Illustrated Reviews)
- It is a potent inhibitor of serotonin reuptake and when used in medium to higher doses also inhibit noradrenaline reuptake. This results in availability of more serotonin and norepinephrine to transmit message between neurons and help to relieve symptoms of depression.
- It has little or no activity at histaminic, alpha- adrenergic and muscarinic receptors.
Pharmacokinetics of Venlafaxine
- It is administered orally and is available in the form of oral tablet or capsule. Both immediate release form and extended-release form are available in market. Patients are advised to take venlafaxine with food to prevent from feeling sick. It is well absorbed after oral administration and its bioavailability is around 45% after oral administration.
- It undergoes extensive first pass metabolism in liver where CYP2D6, CYP3A4 and CYP2C19 isoenzymes play major role in its metabolism. The major metabolite is O- desmethylvenlafaxine (ODV). Mean half-life of venlafaxine is around 5 hours and of ODV is around 11 hours. Both venlafaxine and ODV shows minimum binding with plasma proteins. Some other metabolites like N- desmethylvenlafaxine and N, O- didesmethylvenlafaxine are also formed. However, these metabolites are less active. Venlafaxine and its metabolites are mainly excreted via renal route in the form of urine.
Missed Dose
- If you miss the dose of venlafaxine, take the missed dose as soon as you remember about it. But if it already is time for next dose, skip the missed dose and continue with your regular dosing schedule.
- Avoid taking two doses at a time to make up for the missed dose.
Adverse Effects
- Compared to TCA (Tricyclic Antidepressants), it has lower frequency of sedative and CVS related side effects. However, frequency of GI disturbance, sexual dysfunction and sleep problems are more common with venlafaxine.
- Common side effects of venlafaxine include headache, dizziness, constipation, insomnia, hypotension, abdominal pain etc. It can also cause weight loss, abnormal dreams, seizures, serotonin syndrome, blurred vision, hyponatremia, and impotence.
- US FDA had issued black box warning regarding suicidal risk of venlafaxine.
Drug Interactions
- Concurrent administration with alcohol has additive drowsiness affect so alcohol should be avoided by patients on venlafaxine therapy. It should be used with caution with other CNS sedating drugs. When used with other drugs that increase serotonin level like SSRIs (Selective Serotonin Reuptake Inhibitor), other SNRIs, tramadol etc., it can cause life threatening serotonin syndrome.
- Drugs like ketoconazole, clarithromycin may inhibit metabolism of venlafaxine leading to its accumulation in body. Venlafaxine may decrease effectiveness of metoprolol.
- Concurrent administration with drugs like phentermine may cause excessive weight loss, heart problems and serotonin syndrome. When co-administered with MAO inhibitors which inhibit serotonin metabolism, life threatening serotonin syndrome occur. Hence, venlafaxine should not be taken within 2 weeks of taking MAOIs. Co-administration with cimetidine may increase risk hepatic disease and high blood pressure.
Contraindications/ Warnings
- Contraindicated in patients allergic to venlafaxine. Chances of venlafaxine anaphylaxis (serious allergic reaction) is rare.
- It is only used in patients aged over 18 years and is not approved to be used in those aged 18 years and under.
- It should not be used in patients with glaucoma as it increases intraocular pressure (IOP) in eye.
- Should be used with caution in epileptic patients as it increases risk of seizures.
- Due to its risk of increase in heart rate and blood pressure, it should be used with caution in patients with heart problems and recent myocardial infarction.
- It is used in pregnancy only if absolutely necessary. It passes into breast milk so it should be used by breastfeeding mothers after talking with their doctor.
References
- Linares CL et al. Exploring venlafaxine pharmacokinetic variability with a phenotyping approach, a multicentric french-swiss study (MARVEL study). BMC Pharmacology and Toxicology. 2017; 18(70).
- Ye W wt al. Treatment patterns associated with Duloxetine and Venlafaxine use for Major Depressive Disorder. BMC Psychiatry. 2011; 11(19).
- Gitlin MJ. Venlafaxine, Monoamine Oxidase Inhibitors, and the Serotonin Syndrome. Journal of Clinical Psychopharmacology. 1997; 17(1): 66-67.
- https://www.ncbi.nlm.nih.gov/books/NBK535363/
- https://www.medicalnewstoday.com/articles/263705#precautions
- https://go.drugbank.com/drugs/DB00285
- Lippincott Illustrated Reviews Pharmacology, 6th edition.
- Pharmacology and pharmacotherapeutics. 24th edition.
- Goodman and Gillman Manual of Pharmacology and Therapeutics.