
- Diuretics are drugs which are commonly used to promote diuresis or water loss by increasing urine production. Among various types of diuretics, thiazide and thiazide like diuretics are among most commonly used diuretics.
- Their introduction in 1950s revolutionized the history of oral diuretic therapy. Since then, they have been cornerstone of hypertension treatment. The first approved thiazide diuretics was chlorothiazide in 1958.
- Thiazide organic molecules bi-cyclic structures containing adjacent sulfur and nitrogen atoms on one ring. Thiazide like diuretics don’t have thiazide chemical structure but are pharmacologically like thiazide diuretics. They are least expensive antihypertensive drugs available.
- Some commonly used thiazide and thiazide like diuretics are:
Hydrochlorothiazide
Benzthiazide
Polythiazide
Chlorthalidone
Metolazone
Mechanism of action of Thiazide and Thiazide like Diuretics
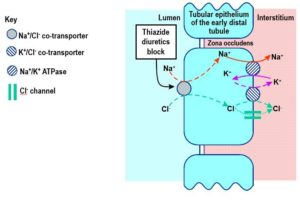
Figure 1- Mechanism of action of Thiazide Diuretics
- They mainly act on distal convoluted tubule (DCT) of nephron and block sodium-chloride transporter (Na+/Cl– transporter). Thus, they inhibit reabsorption of sodium and chloride ions resulting in increased elimination of water from the body.
- As more water is eliminated from body, heart works less to pump blood around the body thus lowering the required blood pressure.
Pharmacological Actions of Thiazide and Thiazide like Diuretics
Diuretic Action
- They cause diuresis with increased excretion of Na+ and Cl– The urine may be very hyperosmolar or concentrated.
- As they increase Na+ concentration in filtrate arriving at distal tubule, more K+ is exchanged with Na+ which causes increased potassium loss with prolonged use of these drugs.
- They decrease Ca+ content in urine by promoting Ca+ reabsorption in urine.
Anti-hypertensive Action
- They possess mild anti-hypertensive action due to reduced peripheral vascular resistance and action on sodium metabolism.
Metabolic Action
- They may cause hyperuricemia, hyperglycemia and hyperlipidemia.
Pharmacokinetics of Thiazide and Thiazide like Diuretics
- They are well absorbed after oral administration. The onset of action starts within 1-2 hours for most thiazides. Most thiazides take 1-3 weeks to produce stable reduction in blood pressure.
- They are distributed throughout ECF (Extra Cellular Fluid) and are concentrated in kidney. They are secreted into tubules and excreted in urine.
- Indapamide, polythiazide and Bendroflumethiazide are primarily metabolized in liver whereas chlorothiazide, hydrochlorothiazide and chlorthalidone are excreted in urine.
- Some of them are long acting because of greater plasma protein binding and high lipid solubility.
- They can cross placental barrier.
| Drug | Oral bioavailability | t1/2 (hours) | Duration of diuretic action hours |
| Chlorothiazide | 9-56% | ̴1.5 | 6-12 |
| Hydrochlorothiazide | ̴70% | ̴2.5 | 12 or more |
| Polythiazide | ̴100% | ̴25 | 24-48 |
| Chlorthalidone | ̴65% | ̴47 | 48 |
| Indapamide | ̴93% | 14 | 24-26 |
Table 1- Pharmacokinetic parameters of different thiazide diuretics
Therapeutic Uses
- As diuretics.
- As anti-hypertensives. They are mainstay of anti-hypertensive medicine as they are easy to administer, inexpensive and well tolerated. Used alone or in combination with other anti-hypertensive agents.
- Useful in treating idiopathic hypercalciuria as they inhibit urinary Ca+
- In nephrogenic diabetes insipidus.
- To treat edema associated with heart, renal and liver disease.
Adverse Effects
- Common side effects are hyponatremia (decreased Na+ concentration), hypokalemia (decreased K+ level) and hypercalcemia (increased Ca+ level). Hypokalemia increases the risk of cardiac arrythmia. In some cases, K+ supplementation may be necessary.
- There are chances of hyperglycemia and hyperuricemia.
- Allergic reaction such as dermatitis and thrombocytopenia my occur due to presence of sulfonamide.
- Other rare side effects include orthostatic hypotension or light headedness (due to volume depletion), impotence in men, GI disturbance, anorexia, headache, weakness and blood dyscrasias.
Drug Interaction
- They may decrease the effects of anticoagulants, uricosuric agents, sulfonylureas and insulin. They increase the effects of anesthetics, diazoxide, cardiac glycosides, lithium, loop diuretics, and vitamin D.
- Their effectiveness may be reduced by NSAIDs and bile acid sequestrants (reduced absorption of thiazides). Amphotericin B and corticosteroids increase the risk of hypokalemia induced by thiazide diuretics.
- Combination with antiarrhythmic drugs may be potentially lethal as it prolongs QT interval. Prolongation of the QT interval lead to the development of polymorphic ventricular tachycardia.
Contraindication
- Contraindicated in hypotension, gout, kidney failure, hypokalemia and lithium therapy.
- Contraindicated in patients allergic to sulphur containing medicines.
- They should be administered in nursing mothers with caution as they can decrease flow of breast milk and can pass into breast milk.
References
- McNally RJ, Morselli F, farukh B, Chowieczyk PJ, Faconti L. A review of the prescribing trend of thiazide-type and thiazide- like diuretics in hypertension: A UK perspective. Br J Clin Pharmacol. 2019; 85: 2707-2713.
- Rapoport RM, Soleimani M. Mechanism of Thiazide Diuretic Arterial Pressure Reduction: The Search Continues. Pharmacol. 2019.
- Moser M, Feig PU. Fifty Years of Thiazide Diuretic Therapy for Hypertension. Arch Intern Med. 2009; 169(20): 1851-1856.
- Lippincott Illustrated Reviews Pharmacology, Edition 6th.
- Pharmacology and pharmacotherapeutics. Edition 24th.
- Goodman and Gillman Manual of Pharmacology and Therapeutics.
- https://www.ncbi.nlm.nih.gov/books/NBK532918/