- Protease inhibitors are a class of anti-viral drugs used to treat HIV/AIDS and hepatitis caused by hepatitis C virus. HIV protease inhibitors were first introduced in 1995 and are effective against both HIV-1 and HIV-2.
- HIV infection is caused by retrovirus that attacks immune system of human being. This retrovirus targets and enters an immune cells inside human body known as T cells and create more HIV viral copies that infect other T cells. Uncontrolled HIV infection lead to AIDS (Acquired Immunodeficiency Syndrome) due to highly impaired immune system.
- HIV protease inhibitors are the 2nd class of antiretroviral drugs developed. The first members of this class, saquinavir, ritonavir and indinavir were approved in late 1995-96.
- Some other protease inhibitors used for HIV treatment include:
- Lopinavir.
- Amprenavir.
- Darunavir.
- Atazanavir.
- Nelfinavir.
- Tipranavir.
Mechanism of action and Resistance
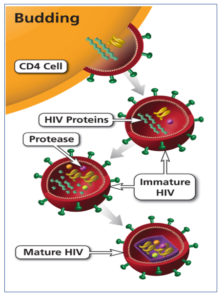
Figure 1- Role of protein in maturation of HIV virus
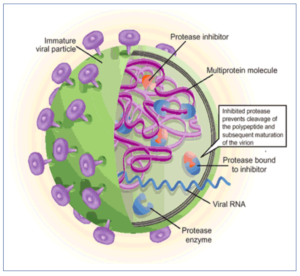
Figure 2- Mechanism of action of Protease Inhibitors
- HIV protease is an enzyme responsible for cleaving viral polyprotein during virion maturation and forming functional proteins. It plays important role in HIV replication. It is aspartyl protease and is a homodimer which consist of two 99-amino-acid monomers.
- HIV protease inhibitors bind reversibly to active site of protease and prevent proteolytic cleavage of viral polyproteins into essential structural and enzymatic components of virus. This prevents maturation of viral particles and results in production of non-infectious virions.
- When an infected patient is treated with HIV protease inhibitors only, plasma HIV RNA concentration decreases by 100-1000 folds within 12 weeks.
- The use of single protease inhibitor may lead to development of resistance. It may be due to mutation in protease active site followed by secondary mutation in site distant than active site.
Therapeutic Uses of protease inhibitors
- Used in combination with other anti-retroviral agents as a part of HAART (Highly Active Anti-Retroviral Therapy) or ‘AIDS cocktail’.
- Ritonavir is used with other PIs as booster regimen.
Pharmacokinetics of protease inhibitors
- They are well absorbed orally. Bioavailability of some PIs like nelfinavir and saquinavir is increased by high-fat diet and bioavailability of indinavir is decreased whereas others are not affected.
- They bound to plasma proteins. Most of them are metabolized by CYP3A4 except nelfinavir which is metabolized predominantly by CYP2C19.
- Most of them inhibit CYP3A4 (ritonavir is more potent). As ritonavir can inhibit CYP3A4, its low dose is used in combination with other PIs to improve their oral bioavailability and prolong their half-life.
- They are extensively metabolized and very small amount is excreted unchanged in urine. They are excreted via bile in the feces. Dosage adjustment are not required in renal impairment.
Adverse Effects
- Common side effects are nausea, vomiting, diarrhea and paresthesia. They may disturb glucose and lipid metabolism and cause diabetes, hypertriglyceridemia and hypercholesterolemia.
- Chronic administration may cause fat redistribution and result in fat accumulation in abdomen and base of neck and loss of fat from extremities.
- Indinavir may cause nephrolithiasis. Jaundice is associated with use of atazanavir.
Drug Interaction
- Due to their property of inhibiting CYP3A4 metabolism, drug interactions are common.
- The drugs which are substrate of CYP3A4 and have narrow therapeutic index may cause dangerous interactions when used with PIs. For example, when used in combination with simvastatin or lovastatin may cause rhabdomyolysis, excessive sedation may occur form midazolam or triazolam and respiratory depression from fentanyl. They may also interact with warfarin, sildenafil and phenytoin.
- Simvastatin and lovastatin are contraindicated with all protease inhibitors.
- The drug which induces CYP 450 enzymes may decrease plasma concentration of PIs. These drugs include rifampin and St. John’s wort (herbal supplement used for depression) and are contraindicated to use with PIs.
- Atazanavir can interact with OTC (Over the Counter) drugs that decrease gastric acid. These drugs include lansoprazole, omeprazole, cimetidine, ranitidine.
References
- Flint OP, Noor MA, Hruz PW, Hylemon PB, Yarasheski K, Donald P. Kotler DP et al. The Role of Protease Inhibitors in the Pathogenesis of HIV-Associated Lipodystrophy: Cellular Mechanisms and Clinical Implications. Toxicol Pathol. 2009; 37(1): 65–77.
- Voshavar C. Protease Inhibitors for the Treatment of HIV/AIDS: Recent Advances and Future Challenges. Curr Top Med Chem. 2019; 19(18): 1571-1598.
- Pharmacology and Pharmacotherapeutics book. 24th edition.
- Goodman and Gillman’s Manual of Pharmacology and Therapeutics.
- Lippincott Illustrated Reviews Pharmacology. 6th edition.
- https://go.drugbank.com/categories/DBCAT000002