
- Diltiazem is non-dihydropyridine calcium channel blocker. Calcium channel blocker (CCBs) also known as calcium channel antagonist or calcium antagonist are group of medicines that block movement of calcium through calcium channel.
- Chemically it is benzothiazepine derivative. It was approved by FDA in 1982. It is also available as generic medicine.
Indications of diltiazem
- Used to treat chronic stable angina.
- In hypertension.
- In atrial arrhythmia.
- To treat paroxysmal supraventricular tachycardia.
- Its off label uses include:
- Migraine prophylaxis.
- Pulmonary hypertension.
- Anal fissures.
- Rest related cramps in lower extremities.
Mechanism of action of diltiazem
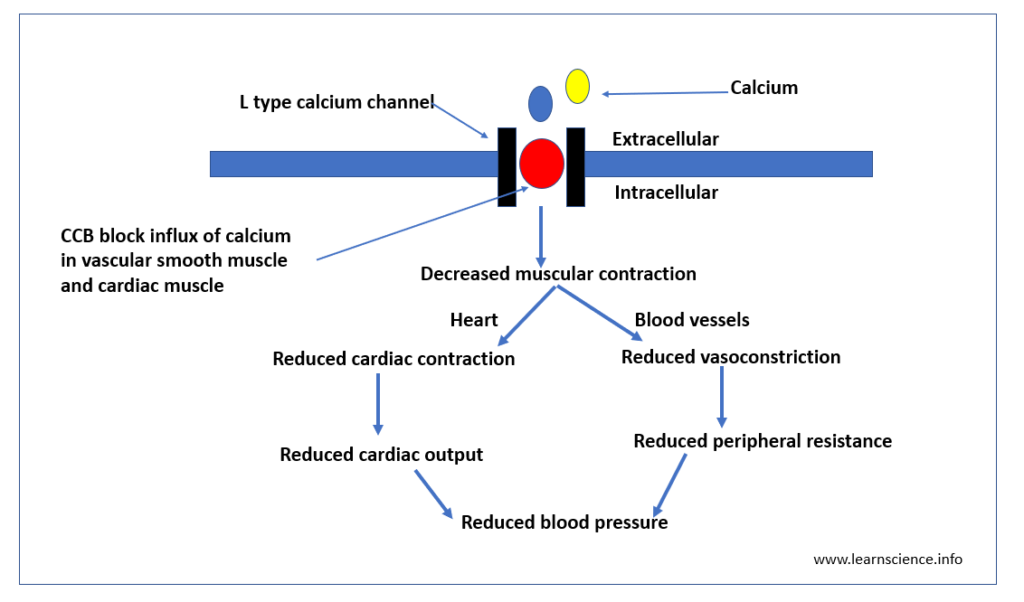
Figure – The primary mechanism of action of diltiazem is by blocking calcium channel
- It exerts its effect by various mechanism of action. Its primary mechanism of action is to inhibit calcium influx by blocking calcium channel.
- Calcium plays important role in excitation-contraction coupling in the skeletal, cardiac and smooth muscle. The contractility of cardiac and vascular smooth muscle is highly dependent on extracellular calcium.
- There are two types of calcium channel in heart: L channel and T channel.
- Diltiazem binds to alpha-1 subunit of L channel and inhibit entry of calcium into cardiac and vascular smooth muscle. This causes decrease in intracellular calcium leading to relaxation of vascular smooth muscle, vasodilation and ultimately reduce blood pressure. It reduces contraction in cardiac muscle and slows sinus pacemaker and AV conduction.
- Diltiazem is potent coronary artery vasodilator. It also exhibits negative ionotropic and negative chronotropic effect.
Pharmacokinetics of diltiazem
- Administered by oral or IV route. Its topical formulation is available for off-label use. It is readily absorbed from GI tract after oral administration. Also available extended-release oral formulation which allows once per day dosing.
- It undergoes extensive first- pass metabolism which is the reason for its low oral bioavailability. It binds extensively to plasma proteins (around 70-80%). The major proteins are albumin and alpha 1 glycoprotein.
- It is metabolized in liver by CYP3A4 enzymes. The major metabolite of diltiazem is N- monodesmethyl diltiazem, deacetyldiltiazem and N- monodesmethyl diltiazem. All the metabolites are less active than diltiazem as vasodilator. It is excreted via urine.
- Its half-life may vary according to the dosage form. The plasma elimination half-life after single or multiple oral dose is 3-4.5 hours, after single or multiple extended release formulation is 6-9 hours and after single IV injection is around 3 hours. Half-life may increase in patients with hepatic impairment.
Adverse Effects
- Its common adverse effects are edema, headache, fatigue, dizziness, and bradycardia. It can also cause severe side effects like congestive heart failure, hepatotoxicity and myocardial infarction.
- It can also create or worsen new arrhythmias.
Drug Interactions
- Concurrent administration of CYP 450 inhibitors may increase its concentration and increase its side effects.
- Concurrent administration of diltiazem with agents which slows cardiac conduction may lead to worsening of side effects like bradycardia or AV block.
- IV diltiazem is contraindicated with concurrent or recent administration of IV beta-blockers as it can cause bradycardia and AV block.
Contraindications
- Contraindicated in patients with hypersensitivity to diltiazem.
- Contraindicated in patients with sick sinus syndrome and second/ third degree AV block.
- IV diltiazem is avoided in patients with cardiogenic shock, ventricular tachycardia, atrial fibrillation or flutter associated with an accessory bypass tract.
References
- https://www.ncbi.nlm.nih.gov/books/NBK532937/
- https://go.drugbank.com/drugs/DB00343
- Padial et al. Clinical Experience with Diltiazem in the Treatment of Cardiovascular Diseases. Cardiol Ther. 2016 Jun; 5(1): 75–82.
- Pharmacology and Pharmacotherapeutics. 24th edition.
- Goodman and Gillman Manual of Pharmacology and Therapeutics.
- Lippincott Illustrated Reviews Pharmacology, 6th edition.
- A Textbook of Clinical Pharmacology and Therapeutics. 5th edition.