
- Cyclosporine is lipophilic cyclic polypeptide which is extracted from the soil fungus Beauveria nivea. It acts as calcineurin inhibitor and has immunosuppressive properties. It was previously known as cyclosprin A.
- Cyclosporine was discovered in lab of Sandoz (now known as Novartis) in 1972 and got its FDA approval for medical use in 1983. It was discovered while searching for novel antifungal agents. Nowadays, it is also synethsized.
Indications of cyclosporine
- Used to prevent and treat organ rejection after solid organ transplantation including organ rejection in liver, kidney, and heart transplant patients.
- In prevention and treatment of graft versus host disease.
- Used to treat several autoimmune diseases including rheumatoid arthritis patient who doesn’t respond to methotrexate.
- To treat severe psoriasis in adult, non-immunocompromised patients who doesn’t respond to at least one systemic therapy.
- Used in amyotrophic lateral sclerosis.
- To treat refractory posterior uveitis.
- Used to treat focal segmental glomerulosclerosis which doesn’t respond to corticosteroids.
- Some of its non-FDA approved indications include
- Autoimmune hepatitis
- Pure red cell aplasia
- Langerhans cell histiocytosis
- Allergic conjunctivitis
- Keratoconjunctivitis
- Atopic dermatitis
- Chronic spontaneous urticaria
- Alopecia areata.
Mechanism of action of cyclosporine
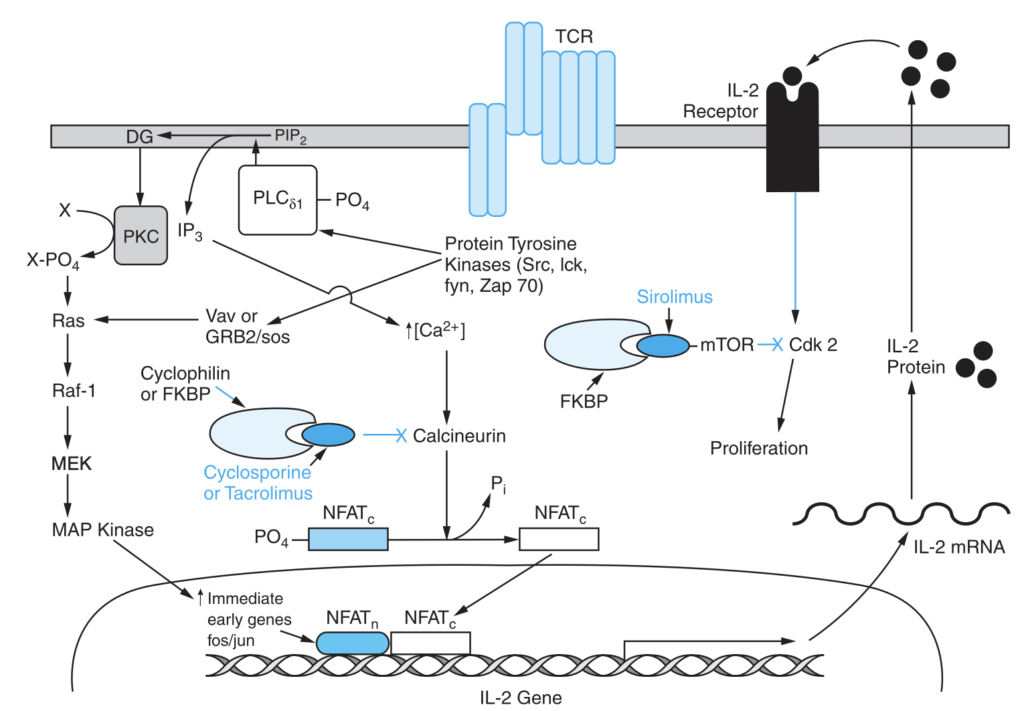
Figure – Mechanism of action of Cyclosporine (Source- Goodman and Gillman Manual of Pharmacology and Therapeutics)
- It is calcineurin inhibitor. Calcineurin is calcium and calmodulin dependent serine/ threonine protein phosphatase and is needed for activating T cells of immune system.
- It first diffuses into T cells, binds to cyclophilin and the complex of cyclosporine- cyclophilin bind to and inhibit calcineurin. Calcineurin in free form causes dephosphorylation of NF-ATc (cytosolic Nuclear Factor of Activated t cells). When it is in complex form, the dephosphorylation of NF-ATc cannot occur which inhibits entry of NF-ATc into nucleus and hence inhibits promotion of reactions required for synthesis of cytokines including IL-2 (interleukin 2). IL-2 plays major role in self- activation and differentiation of T lymphocytes. Hence, the cyclosporine results in immunosuppressant action.
- The main target of cyclosporine is T helper cells. However, it may also suppress T suppressor cells.
Pharmacokinetics of cyclosporine
- It is administered via oral route. IV route is also used. IV preparation need to be dissolved in an ethanol-polyoxyethylated castor oil vehicle. It is mainly absorbed in intestine and its oral bioavailability is around 20-50 %. Oral absorption may vary due to efflux by P- glycoprotein and metabolism by cytochrome P450 isoenzyme in intestine. Its absorption may be delayed and decreased by food. Peak plasma concentration is achieved within 1.5-2 hours of oral administration.
- Around 50 % of drug binds to erythrocytes, 10% to leucocytes and 40% to lipoproteins in plasma. It undergoes extensive metabolism by hepatic CYP3A4. It is metabolized into 25 different metabolites including two hydroxylated (AM-1 and AM-9) and one N- methylated (AM4N) derivative.
- Its half-life is around 8.4- 27 hours. Excretion takes place mainly via feces. It is also excreted in human milk. Dosage adjustment is required in hepatic patients.
Adverse effects
- One of the side effect is nephrotoxicity which occurs in majority of patients and is the major reason for modification or cessation of therapy. It can also cause other side effects including tremor, hirsutism, hypertension, hyperplasia and gum hyperplasia.
- It can cause hyperuricemia which may lead to worsening of gout and can also cause increase in level of LDL cholesterol. Other effects include increased chances of infection, leucopenia, thrombocytopenia, and development of lymphomas caused by Epstein- Barr virus.
Drug Interactions
- As its metabolism depend on CYP3A4, any drugs which affect CYP3A4 may affect blood concentration of cyclosporine. Drugs like antifungal agents (e.g., fluconazole, itraconazole), CCB (calcium channel blocker), glucocorticoids (e.g., methylprednisolone) which inhibit the enzyme CYP3A4 may inhibit the metabolism of cyclosporine and increase its plasma concentration. Some drugs like rifampin, phenytoin, phenobarbital and ticlopidine may induce CYP3A4 and increase metabolism of cyclosporine leading to decreased plasma concentration.
- Concurrent administration of cyclosporine with NSAIDs, other immunosuppressants like tacrolimus, sirolimus and drugs which impair renal function may increase risk of nephrotoxicity. Hence, reduced dose of cyclosporine should be used when used with these agents. Cyclosporine may increase risk of sirolimus induced affects like myelosuppression and hyperlipidemia.
- Grapefruit may inhibit metabolism of cyclosporine by CYP3A4 pathway and may increase its plasma concentration. St. John’s wort may induce CYP3A4 and decrease its plasma concentration.
Contraindication
Contraindicated in following conditions:
- Patients hypersensitive to cyclosporine.
- Patients with active infection.
- In patient with impaired renal function.
- Asthma.
- In patient with uncontrolled hypertension.
- In patient with history of blood dyscrasias.
References
- https://go.drugbank.com/drugs/DB00091
- https://en.wikipedia.org/wiki/Calcineurin
- https://www.ncbi.nlm.nih.gov/books/NBK482450/
- Tedesco D et al. Cyclosporine: A Review. J Transplant. 2012; 2012: 230386.
- Amber T et al. Cyclosporin in dermatology: A practical compendium. 2020; 333(6): e13934.
- Pharmacology and Pharmacotherapeutics. 24th edition.
- Goodman and Gillman Manual of Pharmacology and Therapeutics.
- Lippincott Illustrated Reviews Pharmacology, 6th edition.