
What are tocolytics?
- A normal pregnancy lasts approximately for 40 weeks. Most of the women go into labor during 40th weeks whereas some women may go a little earlier. This condition is called pre-term labor which is characterized by contractions that opens cervix of pregnant women before the 37-week point.
- Tocolytics are medications which are used to suppress pre-mature labor. The word tocolytics is derived from the Greek word ‘tocos’ meaning childbirth and ‘lytics’ meaning capable of dissolving. Tocolytics are also called anti- contraction medications or labor suppressants.
- The factors which may cause pre-term birth may be intrauterine inflammation and infection, precocious fetal endocrine activation, decidual hemorrhage. Preterm birth arises risk of neonatal complications and is the major cause of neonatal mortality and morbidity worldwide and a huge cost burden on healthcare.
- Tocolytic agents can stop uterine contraction and delay delivery for about 48-72 hours. This period allows for transport of the pregnant woman to a perinatal center, and for administration of glucocorticoids like dexamethasone for lung maturation.
Why are tocolytics used?
- To prolong gestation during preterm labor.
- To stop contractions when arranging for caesarean delivery.
- Used to stop contractions in case of spontaneous or induced tachysystole (too many contractions).
Classification of tocolytics
- No tocolytics currently in use was developed specifically to treat preterm labor. The tocolytics used are different classes drugs having other specific use but also can be used as tocolytics.
- Among the most common agents used, as tocolytics are calcium antagonists, β-adrenergic agents, oxytocin antagonists, prostaglandin antagonists, and magnesium sulfate.
Calcium Channel Blocker
- The most commonly used calcium channel blockers as tocolytics are nifedipine and nicardipine. They act by inhibiting calcium influx across cell membranes by blocking L- type voltage dependent calcium channels, thereby decreasing tone in the smooth muscle of the vasculature.
- Numerous randomized clinical trials have shown them to be as effective as beta-mimetics and magnesium in achieving tocolysis.
- Nifedipine may be administered sublingually/orally in the loading dose of 10 mg, and the dose repeated every 20 minutes for 3 doses. Maintenance dose of 10 mg may be given orally every 4-6 hours.
Advantages
- When used for tocolysis, calcium antagonists have fewer maternal side effects than other tocolytics and have no adverse effect on fetal outcome.
- It can be used at any gestational age.
βeta-2 adrenergic agonists
- Selective βeta-2 agonists like salbutamol, ritodrine and terbutaline can be used to delay pre-term labor. They bind with beta-2 receptors on the cell membrane, activate adenlylate cyclase to increase the intracellular concentration of cyclic adenosine monophosphate, resulting in decreased availability of free intracellular calcium for actin and myosin, leading to relaxation of uterine smooth muscle.
- Salbutamol is used by IV infusion in the dose of 10 mcg per minute, gradually increased to 45 mcg per minute until contractions cease; then, the dose is reduced gradually. It can also be administered by IM injection in the initial dose of 100-250 mcg, repeated as necessary.
- Ritodrine is used by IV infusion in the dose of 50 mcg/minute, increased by the same amount once every 20 minutes, until the uterine contractions are controlled and then maintained for an hour thereafter. Then, the lowest dose that maintains uterine quiescence is continued for about 12 hours.
Disadvantages
- Side effects like increased uterine bleeding, hyperglycemia, nausea, tachycardia, pulmonary edema can occur.
- Their effect in significant reduction of neonatal morbidity and mortality hasn’t been convincingly demonstrated.
- They should be contra-indicated in pre-eclampsia (pregnancy complication characterized by high blood pressure and proteins in urine).
COX inhibitors
- Cyclo-oxygenase enzymes convert arachidonic acid (liberated from phospholipid fraction of cell membrane during inflammation, pain or fever) to prostaglandins. Prostaglandins cause uterine contractions when pregnant and non-pregnant. Human decidua, myometrium and fetal membranes express COX-1 enzyme. During labor, there is an intensive increase in COX-2 in the decidua and the myometrium.
- Indomethacin, a nonspecific prostaglandin synthetase inhibitor, when given early, inhibits COX non-selectively and hence inhibit PG synthesis. It is administered orally or as rectal suppositories as a 50 mg loading dose followed by 25-50 mg orally every 6 hours for up to 48 hours. Indomethacin can be used alone or in combination with other tocolytics like magnesium sulphate.
Disadvantages
- It may cause vaginal bleeding, nausea, vomiting and heartburn in mother.
- In fetus, it can cause reduction in amount of urine produced and it can also change the way in which blood circulates through the fetus’s body.
- Indomethacin can also cause ductus arteriosus (blood vessel in developing fetus which connects trunk of pulmonary artery to the proximal descending aorta) to close before the birth of baby. So, it is avoided in gestation of more than 32 weeks. If a pregnant woman takes indomethacin for more than 2 days, ultrasound of baby’s heart should be performed to check the condition of blood vessel.
- It may also increase baby’s risk of developing serious illness like bleeding in the heart, kidney problems, intraventricular hemorrhage (bleeding in the brain), periventricular leukomalacia (a type of brain injury).
Magnesium Sulphate
- Magnesium sulphate is mostly used as 2nd line tocolytics. It acts on the voltage-dependent calcium channels to competitively block the calcium influx, leading to the inhibition of calcium-dependent myosin light-chain kinase phosphorylation and finally inhibiting uterine contraction. Magnesium sulphate is mostly used as adjuvant with Beta-2 adrenergic receptor agonist.
- The current literature on magnesium sulfate in preterm labor presents a mixed picture of risks and benefits. Maternal side effects include flushing, nausea, muscle weakness, chest pain, pulmonary edema, headache, lethargy, dryness of the mouth, blurred vision, transient ischemia, urticarial eruption, maternal hypothermia, and neuromuscular blockade. The effects on the fetus include respiratory and motor depression, decreased muscle tone, and drowsiness in the neonate. According to The American College of Obstetricians and Gynecologists, it is recommended that use of magnesium sulfate as a tocolytic be limited to 48 hours in women from 24 to 34 weeks estimated gestational age.
Oxytocin Receptor Antagonist
- Oxytocin is a potent stimulator of myometrial contractions and play important role in initiation of both term and preterm labor. Atosiban, which is a competitive antagonist of oxytocin can be used as tocolytics. These are primarily licensed to use as tocolytics.
- It is administered through Iv route as 6.75 mg bolus over 1 minute followed by infusion at 18 mg/hour for 3 hours and 6 mg/hour for upto 49 hours. However, due to its excess fetal and infant mortality, when used before 28 weeks of gestation, it is not used nowadays.
Nitric Oxide Donor
- Nitroglycerine IV can delay preterm labor for 48 hours. However, documentation regarding safety, considering its potential effects on the neonatal circulation, is limited.
Antibiotics
- There is increasing evidence that ascending infection by pathogenic organisms may involve the cervix and fetal membranes resulting in the release of prostaglandins, uterine contractility leading to pre-term labor.
- Broad spectrum antibiotic treatment may be effective in reducing the risk of labor progressing to delivery. However, use of prophylactic antibiotic administration before labor has yet to be proven effective.
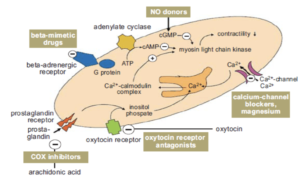
Figure- Overall Mechanism of Action of Tocolytics (Source- https://es.slideshare.net/ankita0809/oxytocics-tocolytics/14)
Some important notes about tocolytics
Till today’s date, there is no 1st line ideal tocolytic as tocolytics may not always prevent pre-term birth. The drugs of first choice are the calcium channel antagonists and oxytocin antagonist. Prostaglandin antagonists have the highest probability of postponing delivery, and have only few maternal side effects, but may have negative effects on the fetus when given after 32 weeks. The efficacies of the various tocolytic agents are comparable to each other and their use depend on factors such as gestational age at the time of tocolytic therapy, amount of cervical dilatation, and degree of effacement, intact or ruptured membranes, and infection. Ideally, tocolytics should not be given for more than 48 hours and should be individualized.
Uses of tocolytics should be contraindicated in certain cases like-
- For prolonging pregnancy in case of chorioamnionitis, fetal death or severe pregnancy induced hypertension.
- In case of anomalous or mature fetus, advanced labor, significant vaginal bleeding, intrauterine growth retardation.
- Beta-adrenergic therapy is contraindicated in case of cardiac diseases, thyrotoxicosis.
- Indomethacin therapy is contraindicated in patients with coagulation disorders, drug-induced asthma, peptic ulcer, hepatic or renal insufficiency.
References
- Callum D. Lamont, Jan Stener Jørgensen & Ronald F. Lamont. The safety of tocolytics used for the inhibition of preterm labour. Expert Opinion Drug Saf. 15(9):1163-1173.
- Bejan-Angoulvant T, Crochet J, Jonville-Bera AP. Calcium channel blockers pharmacology and their use as tocolytics. J Gynecol Obstet Biol Reprod (Paris). 2015 Apr;44(4):305-11.
- Economy KE, Abuhamad AZ. Calcium channel blockers as tocolytics. Semin Perinatol. 2001 Oct;25(5):264-71.
- Vermillion ST, Landen CN. Prostaglandin inhibitors as tocolytic agents. Semin Perinatol. 2001 Aug;25(4):256-62.
- Kawagoe Y, Sameshima H, Ikenoue T, Yasuhi I, Kawarabayashi T. Magnesium sulfate as a second line tocolytic agent for preterm labor: a randomized controlled trial in Kyushu Island. J Pregnancy. Epub 2011 Jun 16. 1-6.
- Dean A, Seehusen, Scott P. Grogan. Magnesium Sulfate for Prevention of Preterm Birth. Am Fam Physician.2015 Apr 1;91(7):444-445.
- López Gómez L, Marín Gabriel MA, Encinas B, de la Cruz Troca JJ, Rodríguez Marrodán B. Oxytocin Receptor Antagonist (Atosiban) in the Threat of Preterm Birth: Does It Have Any Effect on Breastfeeding in the Term Newborn? Breastfeed Med. 2018 Mar;13(2):123-128.
- Drug during pregnancy and lactation. Pages 401-412.
- Drugs during pregnancy and lactation- Page no- 368-380.
- Advances in Organ Biology. Page no- 195-223.
- Pharmacology and Pharmacotherapeutics. Page no- 653-655.