
Introduction
- Chlorpromazine is the first and most famous drug introduced for the treatment of psychosis. It is in the list of essential drugs of World Health Organization (WHO).
- Chlorpromazine was first synthesized in December 1951 in the laboratories of Rhône-Poiulenc. Its introduction in clinical investigation in 1952 by Delay and Deniker revolutionized the treatment of psychiatric disorder.
- Although many new antipsychotic drugs had been discovered, chlorpromazine still remains most commonly used and inexpensive treatment of choice for schizophrenia. It is a benchmark by which other antipsychotic drugs are evaluated by comparing with it.
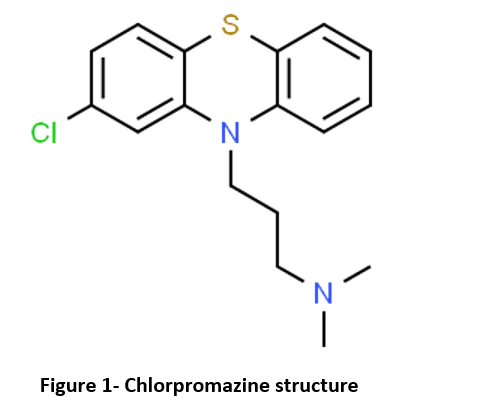
- It is dimethylamine derivative of phenothiazine and belongs to first-generation (typical) antipsychotics.
Mechanism of action of chlorpromazine

- Its precise mechanism of action is not clear.
- It acts by blocking postsynaptic dopamine (D2)receptors and preventing excess of dopamine level in brain. Its efficacy depends on its ability to bind and block dopaminergic receptor in mesolimbic system.
Pharmacological actions of Chlorpromazine
- When given in patients with major psychosis having agitation, it produces psychomotor slowing, emotional quietening and decrease in agitation without producing loss of consciousness. The person becomes silent and don’t respond to external stimuli. chlorpromazine also improves intellectual and cognitive functions and induce sleep in schizophrenics.
- It acts as suppressant of autonomic nervous system. It blocks some action of adrenaline and nor-adrenaline due to alpha adrenergic blocking action. And it also possesses moderate antimuscarinic and anti-5HT actions.
- It also acts as potent antiemetic.
Pharmacokinetics of Chlorpromazine
- Mostly administered through oral or parenteral route. Sometimes it is administered through rectal route. After absorption, they are distributed in whole body tissues. Their concentration in brain is higher than in plasma.
- They are metabolized in liver. An active enterohepatic circulation prolongs the biological half-life of chlorpromazine and its duration of action. Thus, chlorpromazine or its metabolites can be detected in urine even 6 to 12 months after discontinuation of therapy.
Indications of Chlorpromazine
- For treatment of schizophrenia.
- For treating mania, senile psychosis.
- used for treatment of severe behavioral problem in children characterized by hyperexcitable and destructive behavior.
- Used as antiemetic in small, non-sedating dose to control vomiting due to radiation, drugs or uremia. It is also used as antihiccup drug to relieve intractable hiccups.
- For relieving restlessness and apprehension before surgery.
- As an adjunct in treatment of tetanus.
- In acute intermittent porphyria.
Adverse Effects
- Dryness of mouth, palpitation, nasal stuffiness are common.
- It binds to melanin and cause hyperpigmentation of skin, conjunctiva, retina, cornea and lens. Skin eruption, photosensitivity and dermatitis are common. It may cause visual impairment.
- Extrapyramidal symptoms including dystonia, motor restlessness and tardive dyskinesia are dose related. Dystonic symptoms include difficulty in swallowing and breathing, spasm of neck muscles. Motor restlessness includes agitation and insomnia (sometimes). Tardive dyskinesia may occur due to long term therapy or discontinuation of therapy. The symptoms include rhythmic involuntary movement of tongue, face, mouth or jaw.
- Drowsiness may occur during first or second week and then disappear. Postural hypotension, momentary fainting and dizziness are rare after the first oral dose.
- Hematological disorders like agranulocytosis, thrombocytopenia, aplastic anemia is rare. Cholestatic jaundice occur in around 0.5-2% of the cases.
- Abrupt withdrawal of high dose therapy may produce physical dependence like symptoms (nausea, vomiting, gastritis). So, it should be reduced gradually.
Usage in Pregnancy
- Safety for the use of chlorpromazine during pregnancy has not been established. It can cross the placental barrier. So, while prescribing during pregnancy, potential benefits and adverse effects should be compared. In some cases, use of chlorpromazine in third trimester of pregnancy is related to extrapyramidal symptoms, somnolence, feeding disorder in neonates. These complications are varied in different individual. So, it should be prescribed in pregnancy only if potential benefits outweigh its hazards.
- As, it is excreted in breast milk of mothers, a decision should be made whether to discontinue the drug or breastfeeding.
Contraindications
- It should not be used in patients allergic to phenothiazines.
- Should not be used in patients in coma or in presence of large amount of CNS depressants like alcohol and barbiturates.
- Should be used with caution in patients with cardiovascular, hepatic or renal complications. It should be used with caution in patients with glaucoma due to its mydriatic effect.
- It should be discontinued around 48 hours before myelography (An imaging test done in a combination of contrast dye and X rays to detect the disorders with the spinal cord), should not be restarted for at least 24 hours post procedure, and should not be used for the control of nausea and vomiting occurring either prior to myelography or post procedure with metrizamide.
Preparation and Dosage
The commonly used preparations are:
- Chlorpromazine hydrochloride tablets 10, 25, 50 and 100 mg; syrup 25 mg/ml (for adults) and 5 mg/ml (pediatric), and suppositories. Dose 25 mg to 1000 mg.
- Chlorpromazine injection 25 mg/ml. It is usually administered IM in the dose of 25 to 50 mg. The patient should be confined to bed for 30 minutes following IM injection in order to avoid postural hypotension.
Storage
- It should be protected from light to prevent discoloration. Should be stored at 20-25 °C. Protect from freezing.
References
- Adams CE, Rathbone J, Thornley B, Clarke M, Borrill J, Wahlbeck K et al. Chlorpromazine for schizophrenia: a Cochrane systematic review of 50 years of randomized controlled trials. BMC Med. 2005; 3: 15.
- Ban TA. Fifty years chlorpromazine: a historical perspective. Neuropsychiatr Dis Treat. 2007; 3(4): 495–500.
- Retina. 5th edition. Page no- 1532-1554.
- Pharmacology and pharmacotherapeutics. 24th edition.