
- Omeprazole is commonly used proton pump inhibitor (PPI). Over the past several decades, PPIs have become one of the most commonly prescribed medications for peptic ulcer. When compared with earlier agents like systemic and non-systemic antacids, histamine receptor antagonists (H2RAs) and anticholinergics used in management of peptic ulcer, PPIs are quite beneficial as they possess superior acid suppressing capability, consistent patient tolerance and excellent safety.
- Omeprazole is first PPI to be introduced in medical field. Other available PPIs are:
- Pantoprazole
- Lansoprazole
- Rabeprazole.
- It is benzimidazole derivative. It is included in World Health Organization’s List of Essential Medicines and is also available as generic medicine.
Indications of omeprazole
- Used in treatment of duodenal ulcer and gastric ulcer.
- In treatment of Zollinger- Ellison syndrome.
- Treatment and prophylaxis of NSAIDs induced ulcer.
- Treatment of H. pylori infection in combination with antibiotics like clarithromycin, metronidazole and amoxicillin.
Mechanism of action of omeprazole
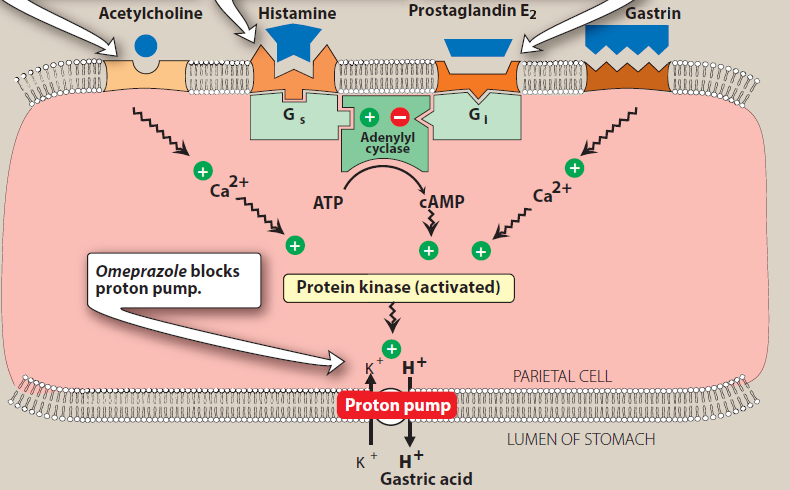
Figure- Mechanism of action of omeprazole (Source- Lippincott’s Illustrated reviews Pharmacology, 6th edition)
- It is a prodrug and require activation at acidic pH. The activated form is absorbed in proximal small intestine, diffuse from blood into the parietal cells and accumulates in the acidic secretory canaliculi. The parietal cell possesses specific hydrogen-potassium-ATPase enzyme (proton pump) which is common final pathway for gastric acid secretion. Omeprazole binds covalently to cysteine residues of the H+-K+-ATPase and inactivate it irreversibly leading to inhibition of gastric acid secretion. The effect last till enzyme is regenerated following stoppage of the drug.
- To prevent premature activation and degradation in luminal gastric acid, it is available in form of enteric coated tablets, gelatin capsules, coated granules as a powder for suspension or in combination with bicarbonates to temporarily neutralize luminal pH.
Pharmacokinetics of omeprazole
- It is administered by oral or parenteral route. It is usually taken half an hour before breakfast and another dose is taken before dinner. The concentration of proton pump molecules is high in parietal cells after fasting for full night, so it is effective when administered before breakfast. As it is acid sensitive, the tablet form should not be crushed or chewed. It should be swallowed whole.
- It is highly protein bound and is metabolized in liver by cytochrome P450 system. The major primary metabolite is 5’ hydroxyomeprazole. The major portion of omeprazole is excreted as metabolites in urine and small amount is excreted in feces.
- Its elimination half-life is around 1 hour. Its single dose may take around 4-5 days to result in maximum reduction in acid production.
Adverse effects
- Generally, it is well tolerated. GI disturbance (vomiting, flatulence, abdominal pain, diarrhea), dizziness and drowsiness may occur.
- Prolonged use and multiple daily doses may increase incidence of osteoporosis. Chronic use of high dose may affect absorption of calcium, magnesium and vitamin B -12. There is evidence that long term use of PPI increases patient’s susceptibility to enteric infections like small intestinal bacterial overgrowth, Salmonella, Campylobacter jejuni, and Clostridium difficile infection.
- It alters bacterial flora of GI tract which may cause malabsorption, enteric infections or acute and chronic lesions in stomach.
Drug Interactions
- It inhibits the hepatic microsomal enzyme and prolongs the half-life of drugs like diazepam, phenytoin, warfarin, carbamazepine etc.
- CYP 450 inducers like rifampicin may cause reduction in concentration of omeprazole.
Contraindication
- Contraindicated in patients with history of hypersensitivity to omeprazole.
- Contraindicated in patients taking rilpivirine.
References
- https://www.statpearls.com/ArticleLibrary/viewarticle/26168
- Howden CW. Drug Disposition Clinical Pharmacology of Omeprazole. Clinical Pharmacokinetics. 1991; 20: 38–49.
- Paz M et al. Pharmacological Effects and Toxicogenetic Impacts of Omeprazole: Genomic Instability and Cancer. Hindawi Oxidative Medicine and Cellular Longevity. 2020; 3457890: 1-21.
- Meyler’s Side Effects of Drugs (Sixteenth Edition). The International Encyclopedia of Adverse Drug Reactions and Interactions. 2016, Pages 647-671.
- Pharmacology and pharmacotherapeutics. 24th edition.
- Goodman and Gillman Manual of Pharmacology and Therapeutics.
- A textbook of clinical pharmacology and therapeutics.
- Lippincott’s Illustrated Reviews Pharmacology. 6th edition.