
- Azathioprine is imidazolyl derivative of 6-mercaptopurine and is a purine antimetabolite. It was first agent to be used in organ transplantation. However, discovery of ciclosporin minimize its use in organ transplantation.
- It was first synthesized in 1956 by William Lange, George Hitching and Gertrude Elion when they were trying to develop derivative of 6- mercaptopurine with better therapeutic index. It is in the World Health Organization’s List of Essential Medicines.
Indications of azathioprine
- For symptomatic treatment of active rheumatoid arthritis.
- as adjunctive therapy in prophylaxis of kidney transplant rejection.
- Its non-FDA approved uses include:
- Inflammatory bowel disease.
- Used in maintenance treatment of autoimmune hepatitis along with steroids.
- Lupus nephritis.
- Multiple sclerosis.
- Severe myasthenia gravis.
- Churg- Strauss syndrome.
- Erythema multiforme.
- Severe and refractory atopic dermatitis.
- In pemphigus vulgaris.
- In maintenance treatment of Crohn disease in children.
Mechanism of action of azathioprine
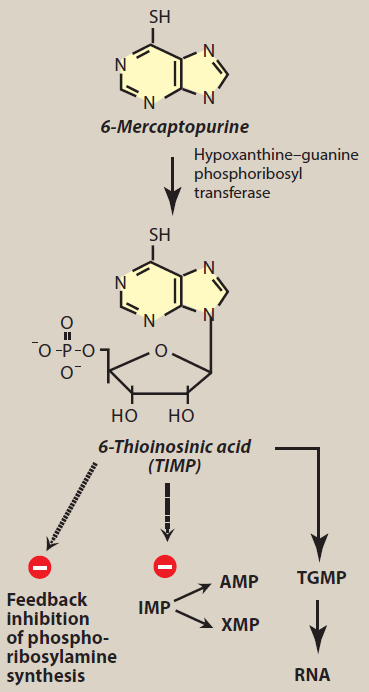
Figure- Azathioprine is converted to 6- mercaptopurine which than exert its immunosuppressant action (IMP- Inosine Monophosphate, AMP- Adenosine Monophosphate, XMP- Xanthine Monophosphate) (source- Lippincott’s Illustrated Reviews Pharmacology, 6th edition)
- It is a prodrug which after administration is converted to its active metabolites, 6- mercaptopurine which is then converted to nucleotide analogue- 6-MP ribose phosphate (6- thioinosinic acid or T-IMP). Hypoxanthine guanine phosphoribosyl transferase (HGPRT) and thiopurine methyltransferase play important role in addition of ribose phosphate group.
- 6-thioinosinic acid inhibit first step of denovo synthesis of purine ring. It inhibits conversion of inosine monophosphate to adenine and guanine nucleotides which are building blocks of RNA and DNA. It is converted to thio-guanine monophosphate which is phosphorylated to di and tri phosphates and incorporated into RNA. Hence, it results in non-functional RNA and DNA and block lymphocyte proliferation and production of interleukin-2 (IL-2) leading to immunosuppression.
Pharmacokinetics of azathioprine
- It is well absorbed after oral administration. It is also administered via IV route. The peak plasma concentration is achieved within 1-2 hours of oral administration. It is administered with food to reduce GI irritation.
- Its half-life is around 10 minutes. Its metabolite 6-MP has half-life of around 1 hour. Both azathioprine and mercaptopurine bind to plasma proteins moderately (around 30%).
- Metabolism take place in liver and exertion occurs via urine. Dosage reduction is required in patients with renal impairment. It doesn’t cross BBB (blood brain barrier).
Adverse effects
- Its major adverse effect is bone marrow suppression including leukopenia, thrombocytopenia, and anemia. Chances of leukopenia is more compared to other two.
- It also increases susceptibility to infections, especially herpes simplex and varicella virus due to its immunosuppressant actions. Other side effects include hepatotoxicity, alopecia, increased risk of neoplasia and alopecia. GI side effects including nausea and vomiting can also occur.
Drug Interactions
- Concurrent administration of azathioprine with drugs like cotrimoxazole, ACE inhibitors or other drugs which cause myelosuppression can cause exaggerated leukopenic response, thrombocytopenia, and anemia.
- Allopurinol inhibits metabolism of azathioprine by inhibiting xanthine oxidase, which is a key enzyme in azathioprine’s metabolism. So, when using these drugs together either its dose should be reduced, or the combination should not be used.
Contraindications
Contraindicated in
- Patients hypersensitive to azathioprine.
- Pregnant or in those who are planning pregnancy. Azathioprine therapy can increase risk of miscarriage, preterm delivery, and low birth weight.
- Contraindicated in patient with active infection.
- In malignancy.
References
- https://www.ncbi.nlm.nih.gov/books/NBK542190/
- https://go.drugbank.com/drugs/DB00993
- Nielsen OH et al. Review article: the treatment of inflammatory bowel disease with 6-mercaptopurine or azathioprine. Aliment Pharmacol Ther. 2001 Nov; 15(11): 1699-708.
- Kidney Transplantation–Principles and Practice (Seventh Edition). 2014, Pages 216-220.
- Pharmacology and Pharmacotherapeutics. 24th edition.
- Goodman and Gillman Manual of Pharmacology and Therapeutics.
- Lippincott Illustrated Reviews Pharmacology, 6th edition.