
- Tricyclic Antidepressants (TCA) are a major category of antidepressants, one of the first ever developed. Although many new antidepressants like SSRIs are developed with fewer side effects, sometimes they fail to work whereas tricyclic antidepressants may work.
- As the name suggests, their structure consist of 3 rings with side chain. They were discovered in early 1950s and marketed later in the decade.
- Some FDA approved tricyclic antidepressants are:
- Amitriptyline
- Nortriptyline
- Protriptyline
- Amoxapine
- Desipramine
- Imipramine
- Doxepin and
- Trimipramine.
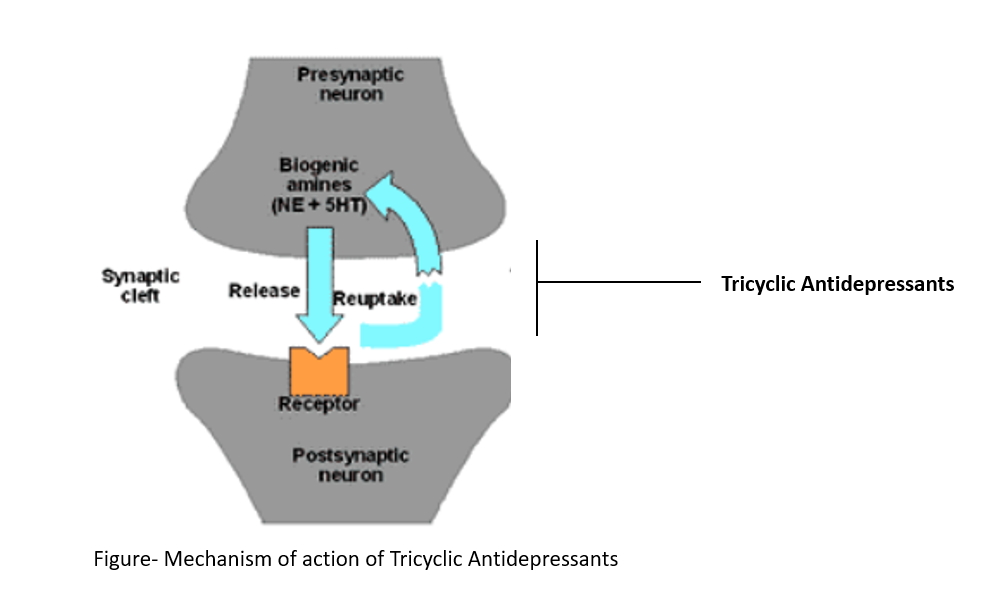
Mechanism of action of tricyclic antidepressants
- Depression is associated with depletion of brain monoamines serotonin (5-HT) and nor-adrenaline (NA). TCAs inhibit neuronal reuptake of nor-adrenaline and serotonin into presynaptic nerve terminals. This results in localized increase in 5-HT/NA in synaptic cleft.
- TCAs also block serotonergic, α-adrenergic, histaminic, and muscarinic receptors. It is responsible for many of adverse effects of TCA.
Pharmacokinetics of tricyclic antidepressants
- All TCAs are rapidly absorbed after oral administration and bind strongly to plasma albumin. They are highly lipophilic so gets distributed throughout the systemic circulation.
- Their metabolism takes place in liver by hepatic microsomal enzymes so may be sensitive to agents that induce or inhibit CYP450 enzymes. Because of their first pass metabolism in liver, they have low and inconsistent bioavailability.
- They are excreted through urine. Peak plasma concentration is at about 2 to 6 hours, and elimination half-life is around 24 hours for most agents, providing a long duration of action.
Uses of tricyclic antidepressants
- To treat major depression.
- To treat acute panic attack, anxiety disorder and social phobias.
- For treatment of obsessive compulsive neurosis (characterized by obsessive pattern of thinking and ritualistic compulsive behavior as defense against anxiety), nocturnal enuresis (involuntary urination in bed while asleep after the age at which bladder control usually begins) and bulimia nervosa (behavioral disorder characterized by overeating, followed by self-induce vomiting or fasting).
- In migraine (amitriptyline is more preferred for this).
- In chronic fatigue syndrome, deafferentation pain and attention deficit hyperactivity disorder (ADHD).
- Low dose of TCAs (doxepin) can be used to treat insomnia.
- In fibromyalgia.
Adverse Effects
- Allergic reactions like pruritus, photo sensitivity, urticaria and skin rashes are observed.
- Antimuscarinic effects are most common and troublesome adverse effects of TCA. These includes dryness of mouth, tachycardia, delayed ejaculation, blurred vision, urinary retention and aggravation of angle-closure glaucoma.
- Long-term therapy may cause postural hypotension, cardiomyopathy and heart failure.
- Weight gain, lethargy, tremors and muscle jerking are observed.
- Amitriptyline, trimipramine, doxepin and imipramine are potent sedatives and can cause sleep compared to other tricyclic antidepressants. So, one should avoid these while doing activities that require alertness like driving.
- Increase in suicidal thoughts or behaviors especially in first few weeks of therapy or after changing doses may occur. So, patients taking antidepressants should be monitored for unusual behavior or worsening depression.
Discontinuation syndrome
- Abrupt discontinuation or unintentionally missed doses may cause discontinuation syndrome in about 40 % of users. Discontinuation syndrome includes nausea, vomiting, dizziness, restlessness, flu-like achiness and insomnia. Rebound depression, panic, anxiety or psychiatric symptoms may occur. The symptoms occur after 2-5 days of discontinuation and may last for 7-14 days.
- Discontinuation syndrome generally occurs after cessation of long-term therapy. Patient should be warned about this and dosage should be reduced gradually while discontinuing therapy.
Contraindications
- They should not be prescribed in patients with cardiac problems like arrythmia, right bundle branch block. They should be used with caution in patients with epilepsy, glaucoma and enlarged prostate.
- In elderly patients, should be used with caution or not at all. Using TCAs during pregnancy may cause suckling problem, jitteriness, hyperexcitability and cardiac arrythmia (rarely) in infants. So, its benefits and adverse effects should be compared while giving to pregnant depressed patients.
- TCAs are dangerous and potentially lethal in overdose, so should not be prescribed in suicidal or impulsive patients.
Overdose is highly dangerous
- Overdose is associated with severe morbidity and death characterized by convulsions, cardiac arrest, and coma (the “3 Cs”). These dangers occur at much higher rates with TCAs than with other antidepressants. Signs and symptoms of toxicity develop rapidly, usually within the first hour of overdose. Manifestations of overdose include prolonged QTc, cardiac arrhythmias, tachycardia, hypertension, severe hypotension, agitation, seizures, central nervous system depression, hallucinations, seizures, and coma.
- Overdose management includes activated charcoal, seizure control, cardioversion, hydration, electrolyte stabilization, and other intensive care.
References
- https://www.mayoclinic.org/diseases-conditions/depression/in-depth/antidepressants/art-20046983
- Schneider J, Patterson M, Jimenez XF. Beyond depression: Other uses for tricyclic antidepressants. Cleveland Clinic Journal of Medicine. 2019; 86 (12): 807-814.
- Gillman PK. Tricyclic antidepressant pharmacology and therapeutic drug interactions updated. Br J Pharmacol. 2007; 151(6): 737–748.
- Kerr GW, McGuffie Ac, Wilkie S. Tricyclic antidepressants overdose: a review. Emerg Med J. 2001; 18: 236–241236.
- Lippincott Illustrated Reviews Pharmacology, 6th edition.
- Pharmacology and pharmacotherapeutics. 24th edition.