
- Sirolimus is macrolide antibiotic obtained from soil mold Streptomyces hygroscopicus. It is used for its immunosuppressant properties.
- Sirolimus is like tacrolimus in structure but have different mechanism of action. It is also known as Rapamycin or Rapamune. It was first isolated in 1972 and got its FDA approval for medical use in September 1999.
Indications of sirolimus
- It is used alone or in combination with other immunosuppressants for prevention and treatment of solid organ transplant and graft versus host rejection (GVH).
- As calcineurin inhibitor like cyclosporine has severe long-term adverse effects, sirolimus is used in withdrawal protocol of calcineurin inhibitor in patients who remain rejection free for first 3 months after organ transplantation.
- It is used topically for uveoretinitis.
- It is also incorporated into stents to inhibit local cell proliferation and blood vessel occlusion.
- To treat lymphangioleiomyomatosis (a rare, progressive lung dsease).
Mechanism of action of sirolimus
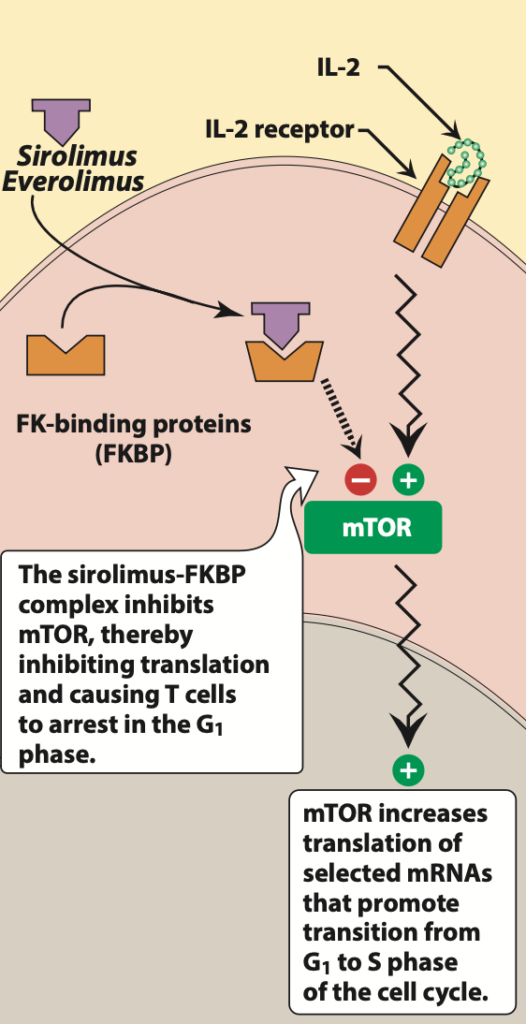
Figure- Mechanism of action of sirolimus (Source- Lippincott’s Illustrated Reviews Pharmacology, 6th edition)
- It inhibits cytokine drive T cell signaling pathway. It first binds to immunophilin, FK binding protein- 12 (FKBP). The sirolimus- FKBP 12 complex doesn’t bind to calcineurin unlike tacrolimus. Instead, this complex binds to and inhibits multifunctional, serine-threonine kinase, mTOR (mammalian target of Rapamycin). mTOR plays important role in various cellular activity like cell cycle progression, DNA repair and regulation of protein translation. Inhibition of mTOR results in blockade of progression of activated T cells from G1 phase to S phase and hence inhibits proliferation of activated T cells. This results in its immunosuppressant activity.
- It is also known as proliferation signal inhibitor (PSI) as it inhibits proliferation of activated T cells.
- Sirolimus doesn’t inhibit production of interleukin 2 (IL 2) unlike tacrolimus and cyclosporine. However, it reduces cellular response to IL 2.
Pharmacokinetics of sirolimus
- Sirolimus is administered orally or via topical route. It is available as oral solution or tablet. It is readily absorbed after oral administration. Absorption may be decreased by high fat meal.
- It has long half-life of around 57- 62 hours, hence once per day dosing is sufficient. Loading dose is require while starting sirolimus therapy. About 40% of sirolimus binds to plasma protein, albumin.
- It is transported by P-glycoprotein and extensively metabolized by CYP3A4. Its metabolites are not active. Major portion is excreted via feces and very small amount is excreted via urine. Dosage adjustment is required in hepatic patients.
Adverse effects
- Some common side effects include myelosuppression, especially thrombocytopenia, diarrhea, hepatoxicity and pneumonitis. It also causes increase in cholesterol and triglyceride level which may require treatment.
- It may cause impaired or delayed wound healing in obese or diabetic patients which may have severe effect immediately after the transplant surgery and in patients who are on corticosteroid therapy. Sirolimus may increase risk of neoplasm and infections.
Drug interactions
- It has synergistic effect when used with cyclosporine. It also increases blood concentration of cyclosporine. Hence, when these two drugs are co-administered, blood level of both drugs should be regularly monitored. This combination also has nephrotoxic effect. Hence, dosage reduction is required when used together.
- As it is substrate of CYP3A4, it may interact with other drugs which inhibit or upregulate CYP3A4 activity. Dose adjustment is required when sirolimus is co- administered with drugs like rifampin and diltiazem.
Contraindication
- Contraindicated in patients with known hypersensitivity to drug.
References
- https://www.pfizermedicalinformation.com/en-us/rapamune/clinical-pharmacology
- https://go.drugbank.com/drugs/DB00877
- Kahan BD. Sirolimus: a comprehensive review. Expert Opin Pharmacother. 2001 Nov;2(11):1903-17.
- LEE VW et al. Sirolimus: Its role in nephrology (Review Article). Nephrology. 2005; 10(6): 606-614.
- Pharmacology and Pharmacotherapeutics. 24th edition.
- Goodman and Gillman Manual of Pharmacology and Therapeutics.
- Lippincott Illustrated Reviews Pharmacology, 6th edition.