
What is epilepsy?
- Epilepsy is a chronic neurological disorder characterized by recurrent seizures associated with disturbance of consciousness and characteristic body movement (convulsion) and sometimes autonomic hyperactivity. A seizure is a sudden, uncontrolled electrical disturbance in the brain. Seizures or black outs have many other causes other than epilepsy like hypoglycemia, migraine, drug withdrawal, cardiac dysrhythmia.
- It affects people of all ages and results in social, economic and behavioral consequences to the patients and their families. It is estimated that more than 50 million people are affected worldwide.
Pathophysiology of epilepsy
- In the late 1800s, Hughlings Jackson suggested that seizures were due to sudden, excessive and uncontrolled discharge of nervous tissue. He envisioned a few cells temporarily becoming highly unstable and inducing surrounding cells to discharge excessively and explosively. The information obtained from modern electrophysiology matches with this.
- To understand in detail about pathophysiology of epilepsy, it is necessary to know about normal physiology of brain.
- In all cells of the body including nerve cells, there is an imbalance in number of positive and negative ions inside and outside the cell due to differences in rate of permeability of those ions through the cell membrane and sodium potassium pump. The inside of the cell is about 70 millivolts more negative than outside which is called the resting membrane potential (R.M.P).
- Excitable tissue such as nerve and muscle owe their excitability to their ability to transmit changes in their R.M.P. Conduction of changes in membrane potential in neuron along its axon cause release of chemical transmitter into synaptic space through which one neuron communicates with other neurons.
- Depending on the neurotransmitter released, brain neurons are classified as excitatory and inhibitory. The primary inhibitory transmitter is GABA (Gamma Amino Butyric Acid) and excitatory transmitter is amino acid glutamate.
- Excitatory transmitter from excitatory neurons cause an increased sodium permeability of next cell’s membrane and causes slight decrease in RMP. This change in membrane potential is called depolarization.
- Similarly, the release of inhibitory neurotransmitter causes an increase in chloride or potassium permeability and causes hyperpolarization.
- An action potential is an ‘all’ or ‘none’ phenomenon; once the threshold is reached, action potential fires. It occurs when there is rapid fall and rise in membrane potential.
- Normally, the neurons fire action potential shortly or in short run and excitability is controlled by powerful inhibitory influences. In normal brain, firing occurs at different time i.e. asynchronously and inhibitory feedback loops regulate the frequency of firing of individual neurons and prevent synchronization.
- When there is defect in inhibitory feedback, a large number of cells in a given area of the brain fire at the same time (i.e. they synchronize) and produce a self-regenerating electrical impulse. Such an area constitutes an epileptic focus. Factors which may trigger the abnormal focus or permit the spread of activity to the normal brain include hyperventilation, alkalosis, hypoglycemia, overhydration, hypocalcemia, overeating, and emotional stress.
- Two important events involved are;
Hyper-excitability:
is the abnormal responsiveness of the neurons to an excitatory input, leading to multiple discharges.
Hypersynchrony:
refers to the recruitment of a large number of nearby neurons to an abnormal firing mode. Thus, epilepsy is a network phenomenon involving the participation of many neurons firing simultaneously.
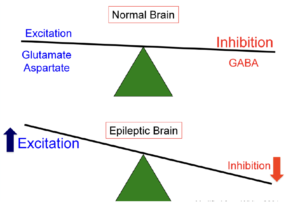
Figure- Pathophysiology of epilepsy (INT- Inhibitory Neurotransmitter, ENT- Excitatory Neurotransmitter)
Types of epilepsy
According to the paper published in 2017 by International League Against Epilepsy (ILAE), the classification of epilepsy has been revised. The types of epilepsy are as follows;
- Generalized seizures
- Focal seizures
- Focal, generalized or unclear epileptic spasm
1. Generalized Seizures:
- In this, the abnormal electrical activity originates simultaneously on both sides of brain and spreads via neuronal network.
Absence seizures:
- It is also known as petitmal seizures. It consists of sudden impairment of consciousness without convulsive movement and without loss of postural control.
- The patient appears to go blank for less than 30 seconds and may be accompanied by subtle signs such as fluttering of eyelids or small chewing movements. The patient may not even know that one has occurred. Absence seizures almost always begin in childhood.
Tonic- clonic seizures:
- They are also known as grandmal or major epilepsy. They are characterized by sudden loss of consciousness, followed by generalized tonic and finally clonic convulsion for about 1-2 minutes. It is followed by period of headache, drowsiness and sleep.
- (Tonic- An increase in muscle contraction, lasting from few seconds to few minutes).
- (Clonic- Symmetrical or asymmetrical jerking of same group of muscles)
Myoclonic seizures:
- This is characterized by a sudden, brief, repetitive muscle contraction involving a body part or the whole body. The whole-body contraction may be followed by violent fall without loss of consciousness.
- Myoclonic seizures may occur by themselves or may coexist with other seizures.
Atonic Seizures:
- This is characterized by sudden loss of postural tone without tonic or clonic movement. The head may drop for few seconds or the child may fall without any apparent cause.
Tonic Seizures:
- It is like tonic-clonic seizures but without clonic phase.
Atonic and tonic seizures are less common generalized seizures than others.
2. Focal Seizures:
- In this, the abnormal electrical activity originates on one side of brain and may or may not spread to other sides of brain. The range of symptoms depend on the site of origin of the abnormal electrical discharge and speed of their spread in brain.
- Awareness may be present, reduced or absent. The abnormal electrical activity can move quickly from a focal seizure to tonic-clonic seizure, affecting both sides and is known as focal to bilateral tonic-clonic seizure.
- In some cases, patient may be conscious and is aware of events which last for few seconds or few minutes like recurrent contraction of muscle group of thumb, toe or angle of mouth. The voluntary control is lost. In some cases, the patient may feel aura (unusual smell, sudden intense emotional feeling) followed by impaired consciousness (30 secs to an hour).
3. Focal and generalized seizures:
- Some people may have both focal and generalized seizures.
Epileptic spasm is seen in neonates and infants and may be due to immature CNS.
Status Epilepticus (SE): Prolonged seizures (more than 5-10 minutes) or repetitive seizures of any type without recovery of consciousness between attacks comprise SE. If tonic-clonic seizure go into SE, the condition may be life-threatening.
References
- Carlos A. M. Guerreiro. Epilepsy: Is there hope? Indian J Med Res. 2016 Nov; 144(5): 657–660.
- Russo ME. The pathophysiology of epilepsy. Cornell Vet. 1981 Apr;71(2):221-47.
- Thijs RD, Surges R, O’Brien TJ, Sander JW. Epilepsy in adults. Lancet. 2019 Feb 16;393(10172):689-701.
- Martin J. Brodie1, Sameer M. Zuberi2, Ingrid E. Scheffer3, Robert S. Fisher4. The2017ILAEclassification of seizure types and the epilepsies: what do people with epilepsy and their caregivers need to know? Epileptic Disord. 2018; 20 (2): 77-87.
- Peter Camfield, Carol Camfield. Incidence, prevalence and aetiology of seizures and epilepsy in children. Epileptic Disord. 2015; 17 (2): 117-123
- Pharmacology and Pharmacotherapeutics. Page no- 141-155.
- A Textbook of Clinical Pharmacology and Therapeutics. 133-141.
- Goodman and Gillman’s Manual of Pharmacology. 319- 335.