
Anti-thyroid Drugs
- Anti-thyroid drugs (ATD) that have major clinical utility are thioureylenes which belong to the family of thioamides. They are used to treat hyperthyroidism caused due to Grave’s disease. They have been in use for over half a century. Thioamides treatment is well accepted by patients and clinicians compared to radioiodine therapy and thyroid surgery.
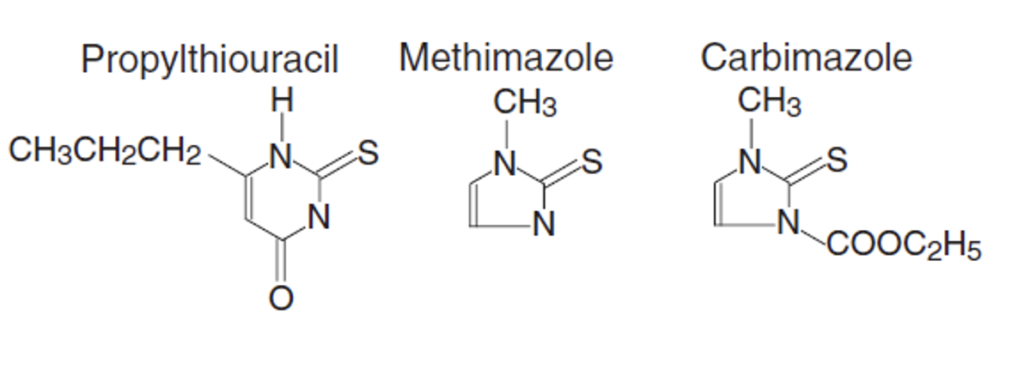
- Commonly used thioamides are propylthiouracil and methimazole. Propylthiouracil and methimazole are used to treat hyperthyroidism in US. In Europe, carbimazole; a carbethexy derivative which is converted to methimazole is also used. Their mechanism of action is similar but have different pharmacokinetics, dosage and adverse effects.
- Thioamides contain sulfhydryl group and thiourea moiety within heterocyclic structure.
Mechanism of action of Anti-thyroid Drugs
- They inhibit thyroid synthesis by inhibiting:
- Coupling of iodotyrosines
- Formation of MIT (Monoiodotyrosine) and conversion of MIT to DIT (Diiodotyrosine).
- Propylthiouracil also inhibit peripheral conversion of T4 (thyroxine) to T3 (triiodothyronine).
Pharmacokinetics of Anti-thyroid Drugs
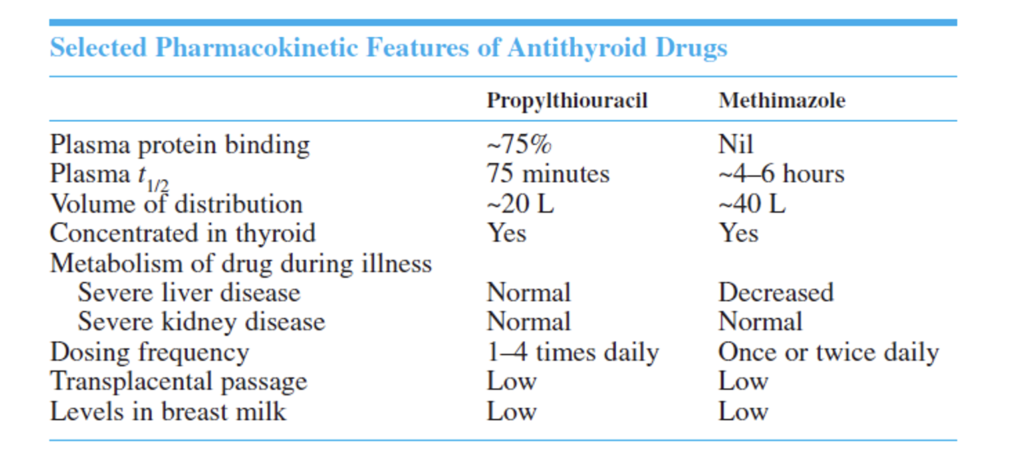
- They are orally administered and rapidly absorbed after oral administration. They are concentrated in thyroid gland. The duration of action of single oral dose is less than 8 hours so they are administered every 6-8 hours. Some physicians may prescribe entire daily dose on a once a day basis.
- Propylthiouracil have shorter half-life compared to methimazole, so it must be dosed more frequently than methimazole.
- They are partly metabolized in thyroid, in liver and partly excreted unchanged in urine.
Uses of Anti-thyroid Drugs
- As initial treatment of hyperthyroidism for one-two years to see if the disease resolves.
- As a short-term treatment to prepare people having Grave’s hyperthyroidism for surgery (thyroidectomy) or radioiodine therapy.
- To treat women with hyperthyroidism during pregnancy.
- To treat hyperthyroidism associated with toxic multinodular goiter or toxic adenoma, usually to prepare for thyroid surgery or radioiodine therapy.
- For long -term treatment of hyperthyroidism due to Grave’s disease in patients who prefer to avoid thyroid surgery or radioiodine therapy.
Adverse Effects
- Most of the side effects are minor, but major side effects can also occur. Both propylthiouracil and methimazole may cause minor side effects like rashes, itching, joint pain and swelling, fever, nausea, vomiting and change in test.
- The major side effects include agranulocytosis which is very rare. It can occur in up to 0.2 % of patients. Development of agranulocytosis is dose related with methimazole but not with propylthiouracil. It develops more commonly within 3 months of starting treatment or can occur later also. Patients should immediately stop taking medicine and consult their physician if signs like sore throat, fever and oral ulceration are observed. It is reversible upon discontinuation of drug.
- Other major side effects include leucopenia, thrombocytopenia, vasculitis (inflammation of blood vessels associated with propylthiouracil) and liver damage (more common with propylthiouracil). Liver damage can be serious and life-threatening. If patients develop jaundice, dark urine, light stools, abdominal pain or other signs of liver dysfunction, they should stop taking medicine and consult their doctors immediately.
Advantages of thioamide drugs
- They are well tolerated and rapidly effective.
- If hypothyroidism occurs, it is reversible.
- Safe to use in children whom radioiodine is contraindicated, and thyroidectomy is technically difficult.
- They can be used during pregnancy (in lowest possible doses).
Disadvantages of thioamide drugs
- Prolonged treatment and follow up are required which may be difficult in case of uneducated or uncooperative patents.
- Recurrence may occur in 20-40 % of cases.
- In patients with severe CHF (Congestive Heart Failure), their action is too slow.
Comparison of methimazole and propylthiouracil
- Methimazole is more effective and helps to maintain euthyroid state much faster than propyl thiouracil. The recurrence rate after withdrawal is comparable in both drugs.
- Methimazole has longer half-life, duration of action and less side effects so it is preferred more than propylthiouracil except in pregnancy during 1st trimester.
- Propylthiouracil is preferred during pregnancy because it causes less severe birth defects than methimazole.
References
- https://www.uptodate.com/contents/antithyroid-drugs-beyond-the-basics#!
- Liu J, Fu J, Xu Y, Wang G. Antithyroid Drug Therapy for Graves’ Disease and Implications for Recurrence. Int J Endocrinol. 2017; 2017: 3813540.
- Cooper DS. Antithyroid Drugs in the Management of Patients with Graves’ Disease: An Evidence-Based Approach to Therapeutic Controversies. The Journal of Clinical Endocrinology & Metabolism. 2003; 88(8): 3474-3481.
- Cooper DS. Antithyroid Drugs. New England Journal of Medicine. 2005; 352(9): 905-17.
- Pharmacology and Pharmacotherapeutics. 24th edition.
- Goodman and Gillman Manual of Pharmacology and Therapeutics.
- Lippincott Illustrated Reviews Pharmacology, 6th edition.