
- Levodopa- the metabolic precursor of dopamine is considered as gold standard treatment for Parkinson’s disease (PD). It is the first drug to be approved for treatment of PD.
- Parkinson’s disease is a slow, progressive neurodegenerative disorder characterized by bradykinesia, rest tremor and postural instability. It is corelated with reduction of dopamine actions in corpus striatum (part of basal ganglia which control motor functions).
- It was introduced for clinical use in Parkinson patients in 1960s. The advantages of adding a dopa decarboxylase inhibitor to treatment were discovered in the early 1970s and the first levodopa combination- carbidopa/levodopa, became commercially available in 1975.
- It is on the WHO (World Health Organization) list of essential medicines.
Mechanism of action of Levodopa
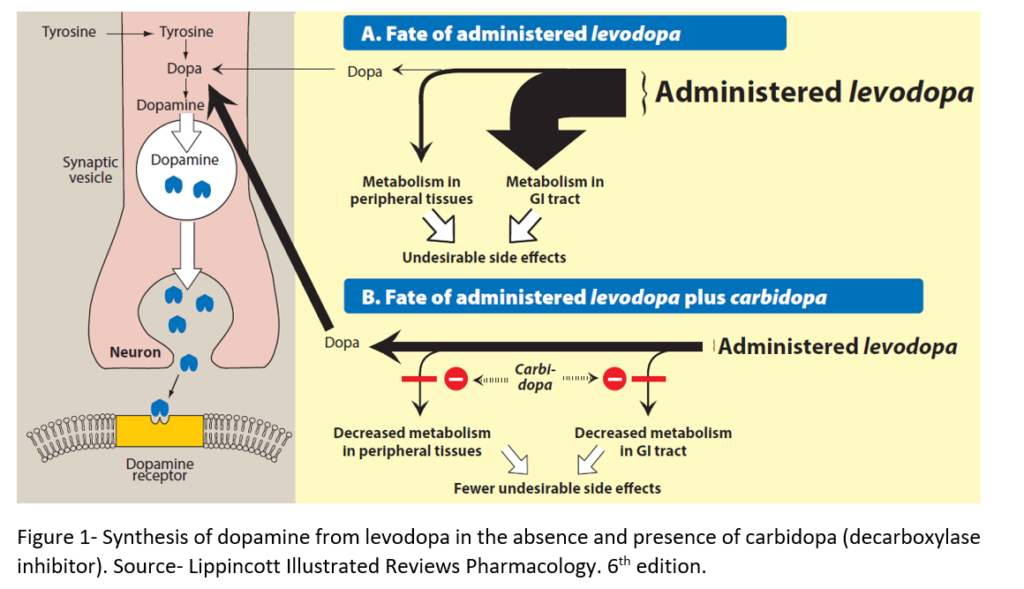
- Dopamine cannot be used to treat PD as it cannot cross BBB (Blood Brain Barrier). Levodopa is a prodrug. It crosses the BBB by an active process and enter nerve terminal in basal ganglia where it is converted to dopamine by decarboxylase enzyme. The dopamine produced is responsible for therapeutic effectiveness.
- When administered alone, it is decarboxylated to dopamine in periphery which causes several side effects and reduce its availability in CNS. Only 1 % of it’s orally administered form reaches the brain. So, it is administered with decarboxylase inhibitors (carbidopa or benserazide) to inhibit metabolism in periphery and increase availability of levodopa in CNS.
- The addition of carbidopa lowers its dose required by 4-5 folds and reduces severity of side effects.
- Decarboxylase inhibitors cannot cross BBB, so they cannot affect conversion of levodopa to dopamine in brain.
Pharmacokinetics of Levodopa
- It is absorbed rapidly from small intestine. The high protein content in meal interfere with absorption of levodopa so it is administered 1 hour before or after food.
- It is widely distributed in blood tissue.
- Its half-life is very short (1-2 hours). Levodopa causes fluctuation in plasma concentration and may give rise to on-off phenomenon or produce fluctuation in motor response.
- It is metabolized by both MAO (Mono-amino Oxidase enzyme) and COMT (Catechol O-Methyl Transferase). It is excreted in urine mainly as metabolite homovanillic acid, partly unchanged and partly as dopamine.
Clinical Uses of Levodopa
- It is used in combination with carbidopa is effective treatment regimen for Parkinson’s disease. This combination decreases rigidity, tremor and other symptoms of PD. It reduces the severity of symptoms in first few years of treatment in approximately two-third patients with PD.
- It improves mood, memory and make the patient more alert. Younger patients with mild symptoms gain more advantage from this drug than elderly patients who cannot tolerate its full dose.
Adverse Effects
- It is generally well tolerated.
- Nausea, vomiting and anorexia are common due to its action on CTZ (Chemoreceptor Trigger Zone). It can cause postural hypotension, tachycardia and mydriasis.
- CNS effects like hallucination, agitation, confusion, restlessness, depression with attempted suicide are observed. Patient with history of psychiatric disturbance should not be treated with levodopa.
- It can cause sedation and sudden onset of sleep. So, driving should be avoided when these effects are seen.
- Abnormal involuntary movement (dyskinesia) may occur on prolonged therapy. They can be quite disturbing and become worse as treatment continues. They may require drug withdrawal.
- It inhibits prolactin secretion and suppress lactation.
- Some patient may show positive Coombs test (antiglobulin test). Saliva and urine become brownish in color because of melanin pigment produced from catechol-amine oxidation.
Drug Interactions
- Administration of levodopa and non-selective MAOI (Mono- amine Oxidase Inhibitors) like phenelzine can cause severe hypertensive crisis (due to increase in catecholamine production). MAOI should be stopped two weeks before starting levodopa therapy.
- Methyldopa promotes adverse effects of levodopa. Vitamin B-6 or pyridoxine reduces efficacy of levodopa by increasing peripheral decarboxylation.
- Reserpine and phenothiazine antagonize effect of levodopa. Antipsychotic drugs are usually contraindicated in PD as they block dopamine receptor and deteriorate parkinsonian symptoms.
Wear-off phenomenon
- Levodopa therapy is associated with ‘wear-off phenomenon’ over the time.
- As the disease progresses, the number of neurons decreases and number of cells which can convert exogenously administered levodopa to dopamine also reduces.
- In wearing off phenomenon, each dose of levodopa improves mobility for certain period (1-2 hours). At the end of dosing interval, rigidity and akinesia return rapidly.
- It can be improved by increasing the dose or frequency of administration. But these may lead to dyskinesia due to high plasma levodopa concentration.
- In the late stages of PD, patients may fluctuate rapidly between being ‘off’- showing no beneficial effects from medications and being ‘on’- but with disabling dyskinesias, a situation called on-off phenomenon.
References
- Monteiro L, Machado AS, Valderramas S, Melo A. The Effect of Levodopa on Pulmonary Function in Parkinson’s Disease: A Systematic Review and Meta-Analysis. Clinical Therapeutics. 2012; 34(5): 1049-1055.
- Dhall R, Kreitzman DL. Advances in levodopa therapy for Parkinson disease Review of RYTARY (carbidopa and levodopa) clinical efficacy and safety. American Academy of Neurology. 2016;86.
- Poulopoulos M, waters C. Carbidopa/levodopa/entacapone: the evidence for its place in the treatment of Parkinson’s disease. Core Evid. 2010; 5: 1–10.
- Tolosa E, Marti MJ, Valldeoriola F, Molinuevo JL. History of levodopa and dopamine agonists in Parkinson’s disease treatment. Neurology. 1998; 50 (6 Suppl 6): S2-10; discussion S44-8.
- https://n.neurology.org/content/86/14_Supplement_1/S13
- Medical Pharmacology and Therapeutics (Fifth Edition). 2018. Page no- 325-336.
- Comprehensive Medicinal Chemistry II. Volume 6. 2007. Page no- 193-228.
- Pharmacology and pharmacotherapeutics. 24th edition.
- Goodman and Gillman’s Manual of Pharmacology.
- A Textbook of Clinical Pharmacology and Therapeutics.
- Lippincott Illustrated Reviews Pharmacology, 6th edition.