
What is histamine?
- Histamine is a potent biogenic amine and acts as chemical messenger. Its name is the combined form of histo- (tissue)+ amine. It is one of the earliest identified allergy mediators.
- Sir Henry Dale and his coworkers isolated histamine from mold ergot and described its properties in 1910. Since than it is one of the most studied amino- acid derived neurotransmitters in CNS (Central Nervous System) and PNS (Peripheral Nervous System).
- Chemically, it consists of an imidazole ring and an amino group connected by two methylene group. It is hydrophilic compound.
Synthesis, Storage and Release of histamine
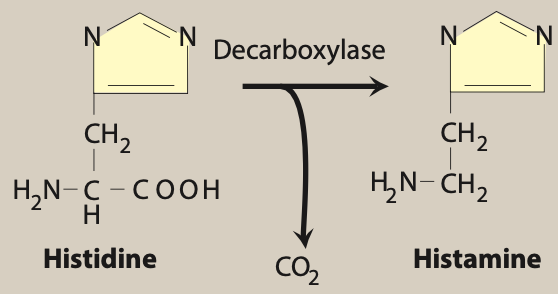
Figure- Synthesis of histamine (Source- Lippincott’s Illustrated Reviews)
- It is synthesized from decarboxylation of amino acid histidine by the enzyme L- histidine decarboxylase. The enzyme L-histidine decarboxylase is present in almost all cells including mast cells, basophils, neuronal cells, and gastric parietal cells. It is also synthesized from dietary histidine by microflora in GI tract.
- It is present in most of the tissues of body including GI tract, lungs, blood vessels and in various biological fluids. Major amount is stored in mast cells and circulating basophils in specialized granules. It is stored in association with chondroitin-4-sulfate in basophils and with anionic proteoglycan heparin in mast cells.
- It is released in response to stimuli like destruction of cells due to cold, toxins or venoms from insects and spiders. It’s release is also triggered by allergy and anaphylaxis. Various therapeutic agents may also induce release of histamine from mast cells. Such agents include succinylcholine, tubocurarine, radiocontrast media and some antibiotics. Vancomycin induced ‘red man syndrome’ may be due to release of histamine.
Mechanism of action
- The released histamine exerts its effect by binding to different histamine receptors. Histamine receptors can be classified into 4 different types: H1, H2, H3 and H4. All these receptors are GPCR (G protein coupled receptors).
| Receptors | H1 | H2 | H3 | H4 |
| Location | Smooth muscle, CNS, endothelial cells | Gastric parietal cells, CNS, mast cells, cardiac muscle | CNS: presynaptic and myenteric plexus | Cells of hematopoietic origin (mainly bone marrow, eosinophil, neutrophils) |
| General role | Itching, pain, hypotension, vasodilation, tachycardia | Increased gastric acidity, increased mucus production in airway, chronotropic, ionotropic action on heart | Prevention of excessive bronchoconstriction, mediate pruritus. | Differentiation of myeloblast and promyelocytes |
| Antagonist | Chlorpheniramine, Fexofenadine, cetirizine | Cimetidine, Ranitidine, Famotidine | Thioperamide,clobenpropit | Thioperamide |
Table- Characteristics of histamine receptors
Pharmacological actions of histamine
Cardiovascular system
- Histamine produces marked vasodilation in human beings. It dilates cerebral blood vessels which can cause throbbing headache and transient increase in CSF pressure.
- When it is injected intradermally, it can induce triple response: Flush which is red line or spot developed within 10 seconds due to local dilation of venules and capillaries, wheal which is local swelling and lasts for around one and half minute and flare in which redness with irregular margins are seen.
Smooth muscle
- It stimulates smooth muscle of various tissues. Its action is more on bronchial and uterine smooth muscle.
Exocrine glands
- It activate H2 receptor present in parietal cell in stomach and play important role in secretion of gastric acid.
CNS (Central Nervous System)
- It is considered as waking amine. H1 and H2 receptors present in brain, when activated by histamine increase sensitivity of large cerebral areas to excitatory inputs. Blockade of histamine receptors in brain by antihistaminic drugs produce drowsiness and sedation.
Immunomodulation
- All four histamine receptors play major role in immunomodulation. Histamine regulates differentiation and activity of B cells, T cells, dendritic cells and monocytes in lymphatic tissues during allergic reactions.
Pathophysiological Role
- Various symptoms of allergy and anaphylactic shock are due to release of various mediators including histamine, leukotriene, serotonin etc. If histamine release is slow and most of the it is inactivated before it reaches blood stream, it can cause local allergic reaction. If it’s release is fast and it reaches blood circulation, full anaphylactoid reaction may occur.
- It’s release is found to be involved in pathophysiology of different autoimmune and allergic disease including urticaria, allergic rhinitis and atopic dermatitis.
Clinical significance
- Various antihistaminic drugs are available to be used for different medical purposes. Many H1 antihistaminic drugs including cetirizine, fexofenadine, dextromethorphan are used in treatment of several allergic disease including chronic urticaria, allergic rhinitis and hay fever. H2 receptor antagonist like ranitidine, cimetidine is used in treatment of peptic ulcer, GERD (Gastric Oesophagul Reflux disease).
- H3 histamine receptor antagonist is under investigation for their role in treating neurodegenerative disease.
Metabolism and Excretion
- It is metabolized by two major pathways, diamine oxidase and histamine N-methyl transferase. It is metabolized to N-methyl histamine by histamine N-methyl transferase which is further converted by MAO (Mono amine oxidase) to N-methylimidazoleeactic acid. Histamine N-methyl transferase is present in airway epithelial cells, intestinal smooth muscle, CNS, liver, and kidneys.
- It undergoes oxidative deamination by diamine oxidase and is converted to imidazoleacetic acid which is further converted to riboside and imidazoleacetic acid. Diamine oxidase is present in liver, kidney, eosinophils, placenta, skin and small intestine mucosa.
References
- https://www.ncbi.nlm.nih.gov/books/NBK557790/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1760721/
- Pharmacology and Pharmacotherapeutics. 24th edition.
- Goodman and Gillman Manual of Pharmacology and Therapeutics.
- Lippincott Illustrated Reviews Pharmacology, 6th edition.
- Essentials of Medical Pharmacology. 7th edition